

Disentangling the effects of a multiple behaviour change intervention for diarrhoea control in Zambia: a theory-based process evaluation
- PMID: 29041941
- PMCID: PMC5645837
- DOI: 10.1186/s12992-017-0302-0
Disentangling the effects of a multiple behaviour change intervention for diarrhoea control in Zambia: a theory-based process evaluation
Abstract
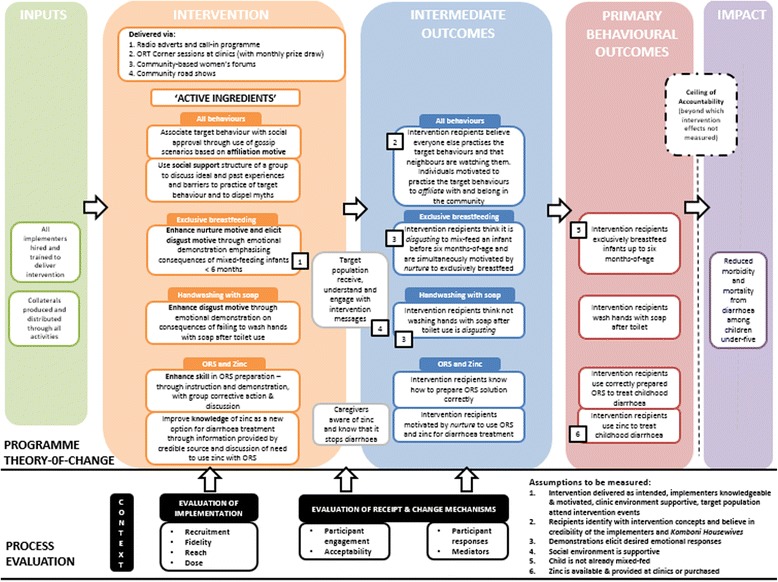
Background: Diarrhoea is a leading cause of child death in Zambia. As elsewhere, the disease burden could be greatly reduced through caregiver uptake of existing prevention and treatment strategies. We recently reported the results of the Komboni Housewives intervention which tested a novel strategy employing motives including affiliation and disgust to improve caregiver practice of four diarrhoea control behaviours: exclusive breastfeeding; handwashing with soap; and correct preparation and use of oral rehydration salts (ORS) and zinc. The intervention was delivered via community events (women's forums and road shows), at health clinics (group session) and via radio. A cluster randomised trial revealed that the intervention resulted in a small improvement in exclusive breastfeeding practices, but was only associated with small changes in the other behaviours in areas with greater intervention exposure. This paper reports the findings of the process evaluation that was conducted alongside the trial to investigate how factors associated with intervention delivery and receipt influenced caregiver uptake of the target behaviours.
Methods: Process data were collected from the eight peri-urban and rural intervention areas throughout the six-month implementation period and in all 16 clusters 4-6 weeks afterwards. Intervention implementation (fidelity, reach, dose delivered and recruitment strategies) and receipt (participant engagement and responses, and mediators) were explored through review of intervention activity logs, unannounced observation of intervention events, semi-structured interviews, focus groups with implementers and intervention recipients, and household surveys. Evaluation methods and analyses were guided by the intervention's theory of change and the evaluation framework of Linnan and Steckler.
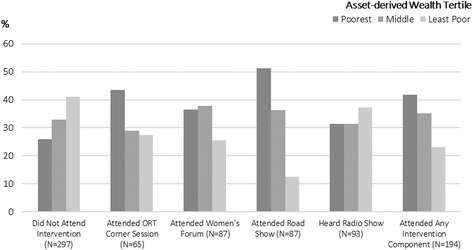
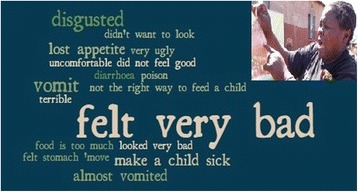
Results: Intervention reach was lower than intended: 39% of the surveyed population reported attending one or more face-to-face intervention event, of whom only 11% attended two or more intervention events. The intervention was not equally feasible to deliver in all settings: fewer events took place in remote rural areas, and the intervention did not adequately penetrate communities in several peri-urban sites where the population density was high, the population was slightly higher socio-economic status, recruitment was challenging, and numerous alternative sources of entertainment existed. Adaptations made by the implementers affected the fidelity of implementation of messages for all target behaviours. Incorrect messages were consequently recalled by intervention recipients. Participants were most receptive to the novel disgust and skills-based interactive demonstrations targeting exclusive breastfeeding and ORS preparation respectively. However, initial disgust elicitation was not followed by a change in associated psychological mediators, and social norms were not measurably changed.
Conclusions: The lack of measured behaviour change was likely due to issues with both the intervention's content and its delivery. Achieving high reach and intensity in community interventions delivered in diverse settings is challenging. Achieving high fidelity is also challenging when multiple behaviours are targeted for change. Further work using improved tools is needed to explore the use of subconscious motives in behaviour change interventions. To better uncover how and why interventions achieve their measured effects, process evaluations of complex interventions should develop and employ frameworks for investigation and interpretation that are structured around the intervention's theory of change and the local context.
Trial registration: The study was registered as part of the larger trial on 5 March 2014 with ClinicalTrials.gov: NCT02081521 .
Keywords: Behaviour change; Breastfeeding; Handwashing; Oral rehydration salts; Process evaluation; Theory of change; Zinc.
Conflict of interest statement
Ethics approval and consent to participate
We obtained written informed consent or a witnessed thumbprint from all participants, regardless of the method. The study protocol was approved by the ethics board at the London School of Hygiene & Tropical Medicine (approval number 6493) and by the University of Zambia Biomedical Research Ethics Committee (ref 001–09-13). The Ministry of Health also gave permission for the study.
Consent for publication
Consent forms specifically stated the following:
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Multiple behaviour change intervention for diarrhoea control in Lusaka, Zambia: a cluster randomised trial.Lancet Glob Health. 2016 Dec;4(12):e966-e977. doi: 10.1016/S2214-109X(16)30262-5. Lancet Glob Health. 2016. PMID: 27855872 Clinical Trial.
-
Theory-based formative research on oral rehydration salts and zinc use in Lusaka, Zambia.BMC Public Health. 2016 Apr 12;16:312. doi: 10.1186/s12889-016-2984-2. BMC Public Health. 2016. PMID: 27067003 Free PMC article. Clinical Trial.
-
Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Kenya: a cluster-randomised controlled trial.Lancet Glob Health. 2018 Mar;6(3):e316-e329. doi: 10.1016/S2214-109X(18)30005-6. Epub 2018 Jan 29. Lancet Glob Health. 2018. PMID: 29396219 Free PMC article. Clinical Trial.
-
Hand-washing promotion for preventing diarrhoea.Cochrane Database Syst Rev. 2021 Jan 6;12(1):CD004265. doi: 10.1002/14651858.CD004265.pub4. Cochrane Database Syst Rev. 2021. PMID: 33539552 Free PMC article.
-
Interventions for supporting the initiation and continuation of breastfeeding among women who are overweight or obese.Cochrane Database Syst Rev. 2019 Sep 17;9(9):CD012099. doi: 10.1002/14651858.CD012099.pub2. Cochrane Database Syst Rev. 2019. PMID: 31529625 Free PMC article.
Cited by
-
Effectiveness of hygiene kit distribution to reduce cholera transmission in Kasaï-Oriental, Democratic Republic of Congo, 2018: a prospective cohort study.BMJ Open. 2021 Oct 14;11(10):e050943. doi: 10.1136/bmjopen-2021-050943. BMJ Open. 2021. PMID: 34649847 Free PMC article.
-
Exclusive breastfeeding lowers the odds of childhood diarrhea and other medical conditions: evidence from the 2016 Ethiopian demographic and health survey.Ital J Pediatr. 2021 Aug 3;47(1):166. doi: 10.1186/s13052-021-01115-3. Ital J Pediatr. 2021. PMID: 34344434 Free PMC article.
-
Process Evaluation of "The Hygienic Family" Intervention: A Community-Based Water, Sanitation, and Hygiene Project in Rural Malawi.Int J Environ Res Public Health. 2022 Jun 1;19(11):6771. doi: 10.3390/ijerph19116771. Int J Environ Res Public Health. 2022. PMID: 35682353 Free PMC article.
-
Improving child health service interventions through a Theory of Change: A scoping review.Front Pediatr. 2023 Apr 6;11:1037890. doi: 10.3389/fped.2023.1037890. eCollection 2023. Front Pediatr. 2023. PMID: 37090921 Free PMC article.
-
Distribution of hygiene kits during a cholera outbreak in Kasaï-Oriental, Democratic Republic of Congo: a process evaluation.Confl Health. 2020 Jul 24;14:51. doi: 10.1186/s13031-020-00294-w. eCollection 2020. Confl Health. 2020. PMID: 32760439 Free PMC article.
References
-
- Coryn C, Noakes L, Westine C, Schroter D. A systematic review of theory-driven evaluation practice from 1990 to 2009. Am J Eval. 2011;32:199–226. doi: 10.1177/1098214010389321. - DOI
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
