

Pisa syndrome in Parkinson's disease: electromyographic quantification of paraspinal and non-paraspinal muscle activity
- PMID: 29042003
- PMCID: PMC5726350
- DOI: 10.11138/fneur/2017.32.3.143
Pisa syndrome in Parkinson's disease: electromyographic quantification of paraspinal and non-paraspinal muscle activity
Abstract
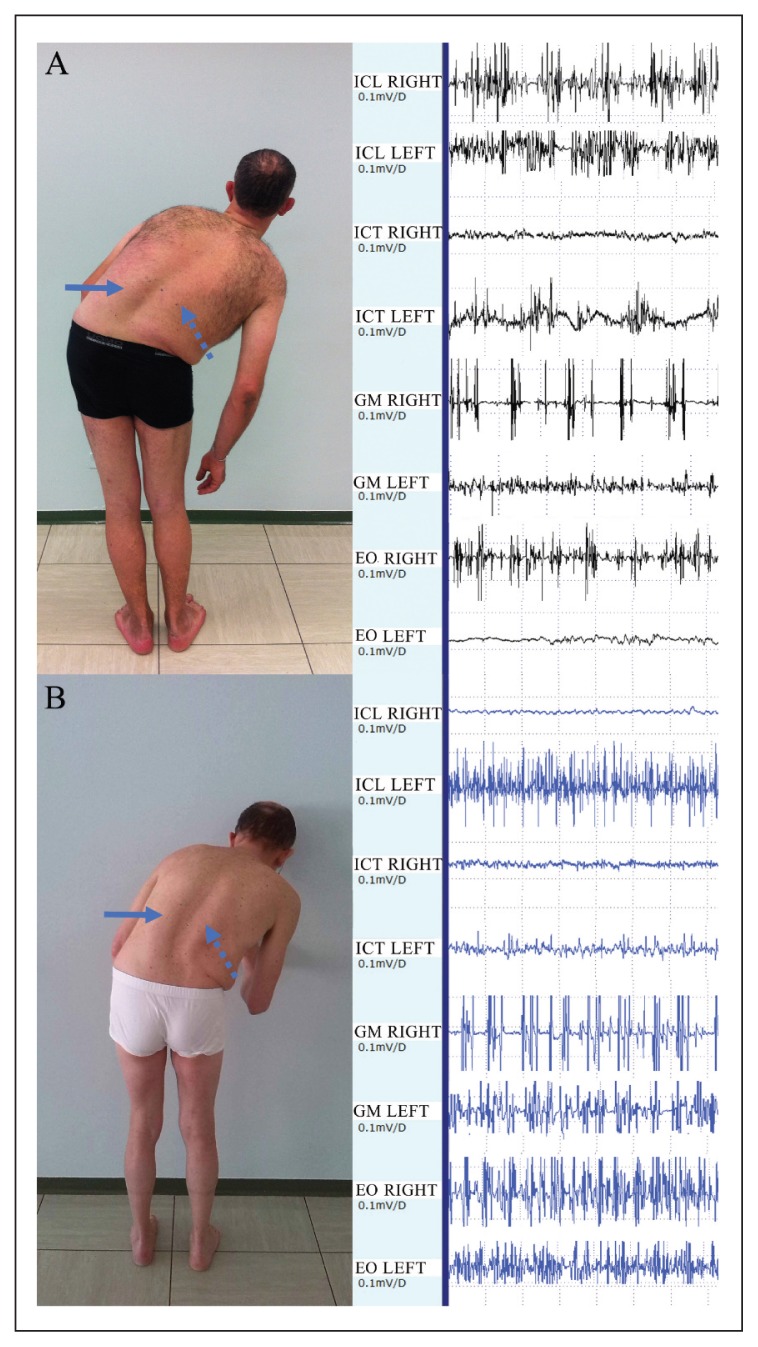
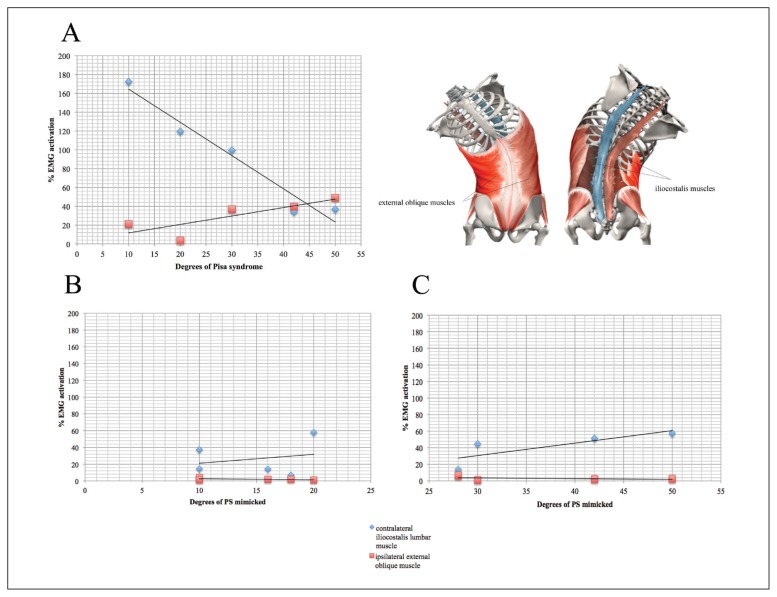
Patients with Parkinson's disease (PD) and Pisa syndrome (PS) may present tonic dystonic or compensatory (i.e. acting against gravity) hyperactivity in the paraspinal and non-paraspinal muscles. Electromyographic (EMG) activity was measured in nine patients with PD and PS, three with PD without PS, and five healthy controls. Fine-wire intramuscular electrodes were inserted bilaterally into the iliocostalis lumborum (ICL), iliocostalis thoracis (ICT), gluteus medius (GM), and external oblique (EO) muscles. The root mean square (RMS) of the EMG signal was calculated and normalized for each muscle. In stance condition, side-to-side muscle activity comparisons showed a higher RMS only for the contralateral ICL in PD patients with PS (p=0.028). Moreover, with increasing degrees of lateral flexion, the activity of the EO and the ICL muscles progressively increased and decreased, respectively. The present data suggest that contralateral paraspinal muscle activity plays a crucial compensatory role and can be dysfunctional in PD patients with PS.
Figures
Similar articles
-
Pisa syndrome in Parkinson's disease: an electrophysiological and imaging study.J Neurol. 2013 Aug;260(8):2138-48. doi: 10.1007/s00415-013-6945-8. Epub 2013 May 22. J Neurol. 2013. PMID: 23695587
-
Pisa syndrome in Parkinson's disease: clinical, electromyographic, and radiological characterization.Mov Disord. 2012 Feb;27(2):227-35. doi: 10.1002/mds.23930. Epub 2011 Oct 13. Mov Disord. 2012. PMID: 21997192
-
Botulinum toxin for Pisa syndrome: An MRI-, ultrasound- and electromyography-guided pilot study.Parkinsonism Relat Disord. 2019 May;62:231-235. doi: 10.1016/j.parkreldis.2018.11.003. Epub 2018 Nov 5. Parkinsonism Relat Disord. 2019. PMID: 30442481
-
Trunk muscle activation pattern in parkinsonian camptocormia as revealed with surface electromyography.Parkinsonism Relat Disord. 2017 Nov;44:44-50. doi: 10.1016/j.parkreldis.2017.08.028. Epub 2017 Aug 31. Parkinsonism Relat Disord. 2017. PMID: 28882381
-
Lateral flexion in Parkinson's disease and Pisa syndrome.J Neurol. 2006 Dec;253 Suppl 7:VII17-20. doi: 10.1007/s00415-006-7005-4. J Neurol. 2006. PMID: 17131222 Review.
Cited by
-
Botulinum Toxin for Axial Postural Abnormalities in Parkinson's Disease: A Systematic Review.Toxins (Basel). 2024 May 15;16(5):228. doi: 10.3390/toxins16050228. Toxins (Basel). 2024. PMID: 38787080 Free PMC article.
-
Does the Degree of Trunk Bending Predict Patient Disability, Motor Impairment, Falls, and Back Pain in Parkinson's Disease?Front Neurol. 2020 Mar 31;11:207. doi: 10.3389/fneur.2020.00207. eCollection 2020. Front Neurol. 2020. PMID: 32296383 Free PMC article.
-
Gait Analysis in Parkinson's Disease: An Overview of the Most Accurate Markers for Diagnosis and Symptoms Monitoring.Sensors (Basel). 2020 Jun 22;20(12):3529. doi: 10.3390/s20123529. Sensors (Basel). 2020. PMID: 32580330 Free PMC article. Review.
References
-
- Adams MA, Dolan P, Hutton WC. Diurnal variations in the stresses on the lumbar spine. Spine (Phila Pa) 1987;1976;12:130–137. - PubMed
-
- Beith ID, Harrison PJ. Stretch reflexes in human abdominal muscles. Exp Brain Res. 2004;159:206–213. - PubMed
-
- Bonanni L, Thomas A, Varanese S, et al. Botulinum toxin treatment of lateral axial dystonia in Parkinsonism. Mov Disord. 2007;22:2097–2103. - PubMed
-
- D’Antona G, Pellegrino MA, Carlizzi CN, et al. Deterioration of contractile properties of muscle fibres in elderly subjects is modulated by the level of physical activity. Eur J Appl Physiol. 2007;100:603–611. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical