

Optimal blood pressure during cardiopulmonary bypass defined by cerebral autoregulation monitoring
- PMID: 29042040
- PMCID: PMC5685671
- DOI: 10.1016/j.jtcvs.2017.04.091
Optimal blood pressure during cardiopulmonary bypass defined by cerebral autoregulation monitoring
Abstract
Objectives: We sought to define the lower and upper limits of cerebral blood flow autoregulation and the optimal blood pressure during cardiopulmonary bypass. We further sought to identify variables predictive of these autoregulation end points.
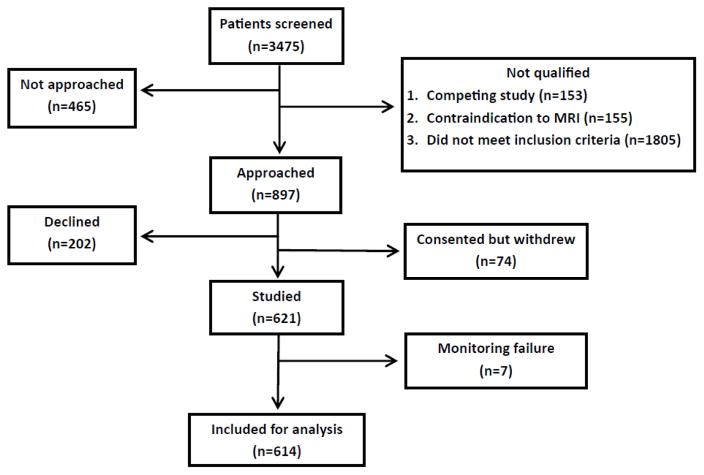
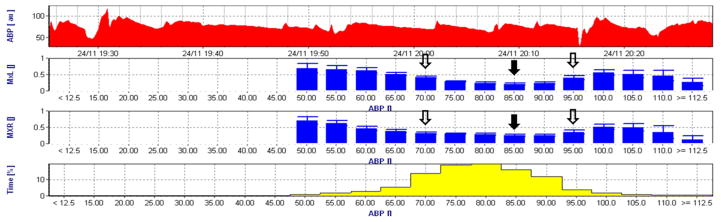
Methods: Cerebral autoregulation was monitored continuously with transcranial Doppler in 614 patients during cardiopulmonary bypass enrolled in 3 investigations. A moving Pearson's correlation coefficient was calculated between cerebral blood flow velocity and mean arterial pressure to generate the variable mean velocity index. Optimal mean arterial pressure was defined as the mean arterial pressure with the lowest mean velocity index indicating the best autoregulation. The lower and upper limits of cerebral blood flow autoregulation were defined as the mean arterial pressure at which mean velocity index was increasingly pressure passive (ie, mean velocity index ≥0.4) with declining or increasing blood pressure, respectively.
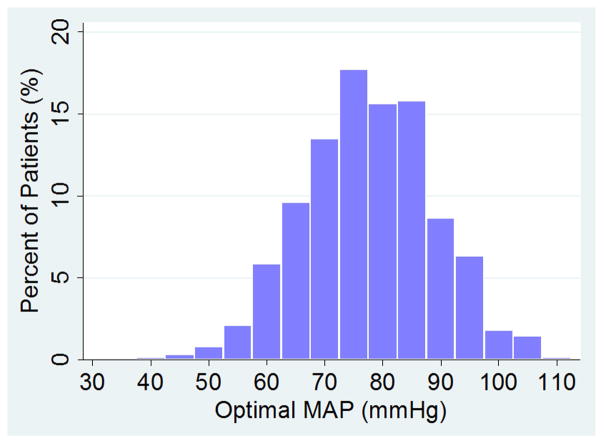
Results: The mean (± standard deviation) lower and upper limits of cerebral blood flow autoregulation, and optimal mean arterial pressure were 65 ± 12 mm Hg, 84 ± 11 mm Hg, and 78 ± 11 mm Hg, respectively, after adjusting for study enrollment. In 17% of patients, though, the lower limit of cerebral autoregulation was above this optimal mean arterial pressure, whereas in 29% of patients the upper limit of autoregulation was below the population optimal mean arterial pressure. Variables associated with optimal mean arterial pressure based on multivariate regression analysis were nonwhite race (increased 2.7 mm Hg; P = .034), diuretics use (decreased 1.9 mm Hg; P = .049), prior carotid endarterectomy (decreased 5.5 mm Hg; P = .019), and duration of cardiopulmonary bypass (decreased 1.28 per 60 minutes of cardiopulmonary bypass). The product of the duration and magnitude that mean arterial pressure during cardiopulmonary bypass was below the lower limit of cerebral autoregulation was associated with the risk for stroke (P = .02).
Conclusions: Real-time monitoring of autoregulation may improve individualizing mean arterial pressure during cardiopulmonary bypass and improving patient outcomes.
Keywords: blood pressure; cardiopulmonary bypass; cerebral autoregulation.
Copyright © 2017 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: Dr. Hogue receives consulting fees, lecture honorarium, and research funding from Medtronics, Inc, Minneapolis, MN.
Figures
Comment in
-
Chasing the elusive cerebral autoregulation curve in pursuit of intraoperative brain protection.J Thorac Cardiovasc Surg. 2017 Nov;154(5):1599-1600. doi: 10.1016/j.jtcvs.2017.05.055. Epub 2017 May 24. J Thorac Cardiovasc Surg. 2017. PMID: 28623095 No abstract available.
-
Optimizing cerebral blood flow: Hitting the sweet spot on cardiopulmonary bypass.J Thorac Cardiovasc Surg. 2017 Nov;154(5):1588-1589. doi: 10.1016/j.jtcvs.2017.05.032. Epub 2017 May 19. J Thorac Cardiovasc Surg. 2017. PMID: 28629838 No abstract available.
-
Discussion.J Thorac Cardiovasc Surg. 2017 Nov;154(5):1597-1598. doi: 10.1016/j.jtcvs.2017.04.095. J Thorac Cardiovasc Surg. 2017. PMID: 29042041 No abstract available.
-
Targeting optimal blood pressure monitoring: what's next?J Thorac Dis. 2018 Sep;10(Suppl 26):S3281-S3285. doi: 10.21037/jtd.2018.08.115. J Thorac Dis. 2018. PMID: 30370138 Free PMC article. No abstract available.
References
-
- Gibbon JH., Jr Application of a mechanical heart and lung apparatus to cardiac surgery. Minn Med. 1954;37:171–185. passim. - PubMed
-
- Hannan EL, Wu C, Walford G, et al. Drug-eluting stents vs. coronary-artery bypass grafting in multivessel coronary disease. N Engl J Med. 2008;358:331–341. - PubMed
-
- Hogue CW, Jr, Palin CA, Arrowsmith JE. Cardiopulmonary bypass management and neurologic outcomes: an evidence-based appraisal of current practices. Anesth Analg. 2006;103:21–37. - PubMed
-
- Murkin JM, Farrar JK, Tweed WA, McKenzie FN, Guiraudon G. Cerebral autoregulation and flow/metabolism coupling during cardiopulmonary bypass: the influence of PaCO2. Anesth Analg. 1987;66:825–832. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
