

Effects of dietary nitrate on respiratory physiology at high altitude - Results from the Xtreme Alps study
- PMID: 29042272
- PMCID: PMC5687938
- DOI: 10.1016/j.niox.2017.10.005
Effects of dietary nitrate on respiratory physiology at high altitude - Results from the Xtreme Alps study
Abstract
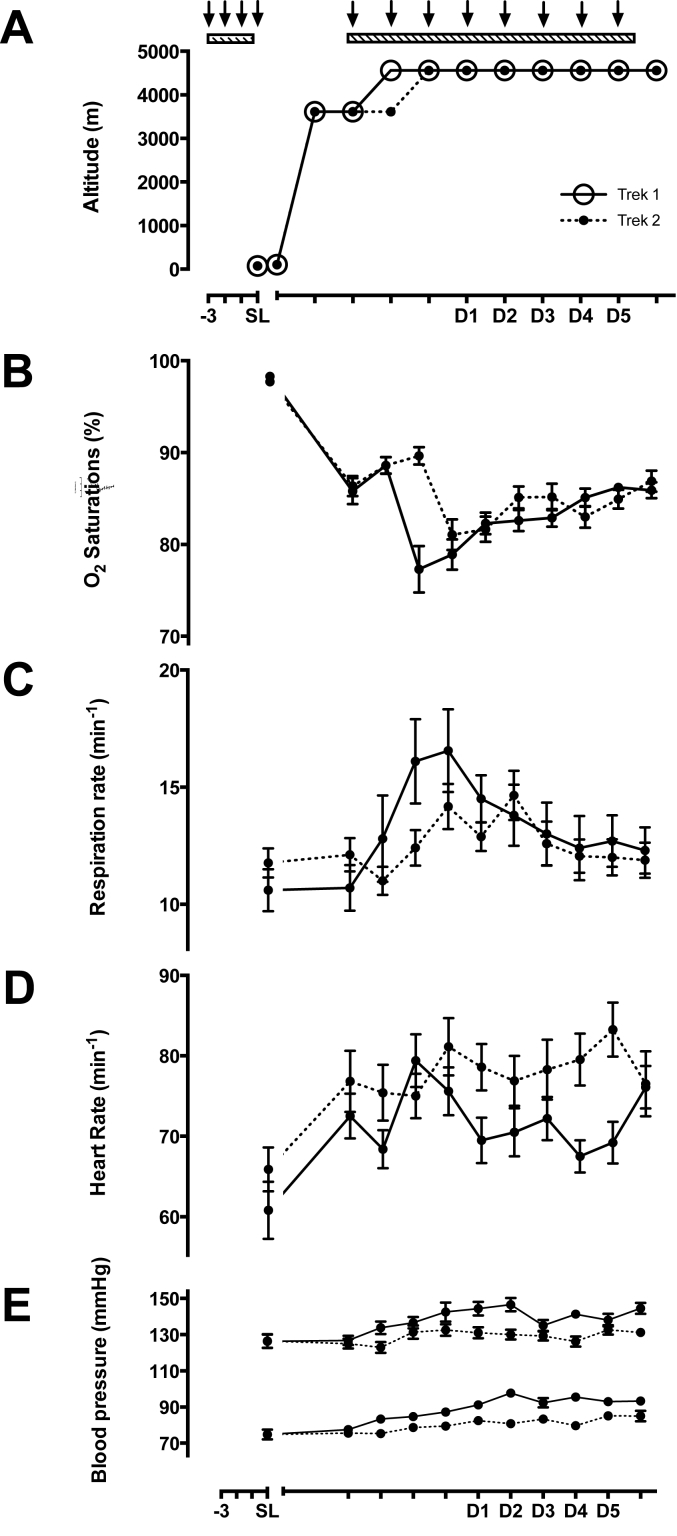
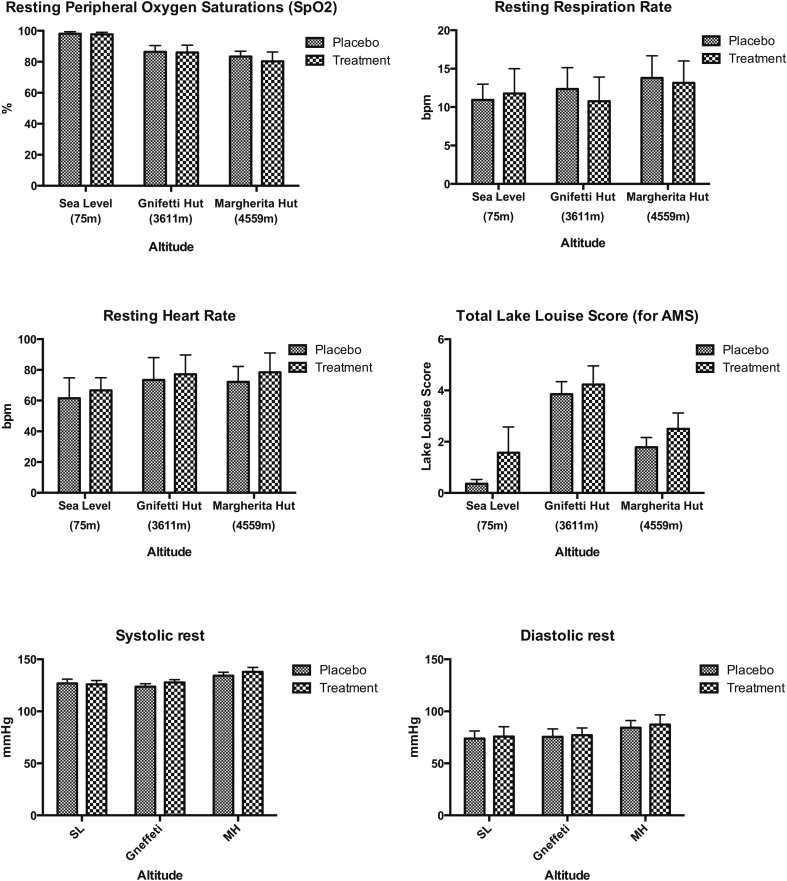
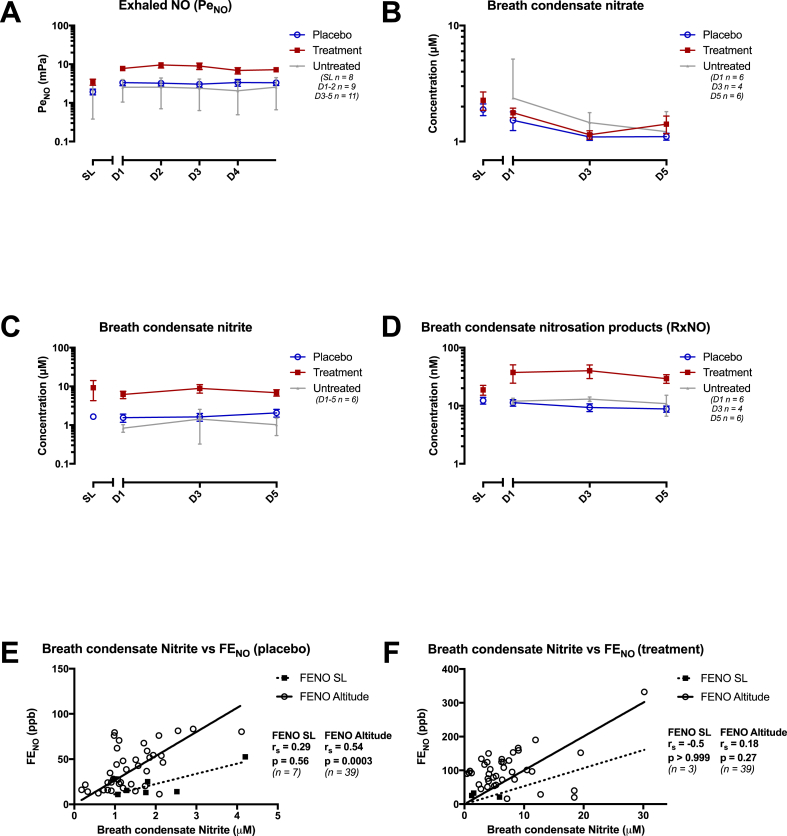
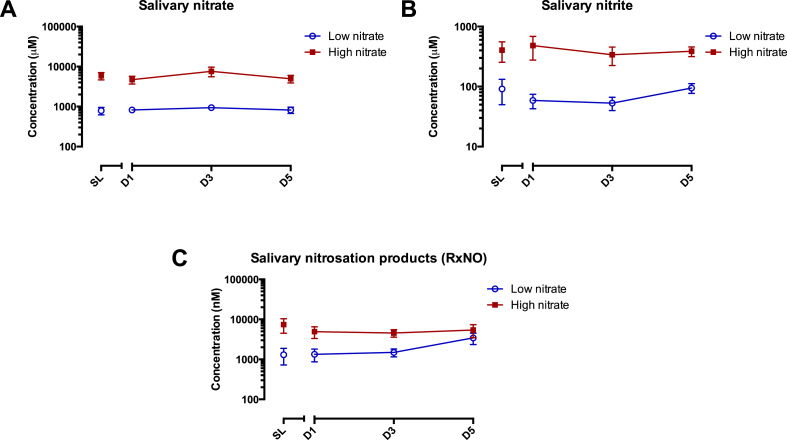
Nitric oxide (NO) production plays a central role in conferring tolerance to hypoxia. Tibetan highlanders, successful high-altitude dwellers for millennia, have higher circulating nitrate and exhaled NO (ENO) levels than native lowlanders. Since nitrate itself can reduce the oxygen cost of exercise in normoxia it may confer additional benefits at high altitude. Xtreme Alps was a double-blinded randomised placebo-controlled trial to investigate how dietary nitrate supplementation affects physiological responses to hypoxia in 28 healthy adult volunteers resident at 4559 m for 1 week; 14 receiving a beetroot-based high-nitrate supplement and 14 receiving a low-nitrate 'placebo' of matching appearance/taste. ENO, vital signs and acute mountain sickness (AMS) severity were recorded at sea level (SL) and daily at altitude. Moreover, standard spirometric values were recorded, and saliva and exhaled breath condensate (EBC) collected. There was no significant difference in resting cardiorespiratory variables, peripheral oxygen saturation or AMS score with nitrate supplementation at SL or altitude. Median ENO levels increased from 1.5/3.0 mPa at SL, to 3.5/7.4 mPa after 5 days at altitude (D5) in the low and high-nitrate groups, respectively (p = 0.02). EBC nitrite also rose significantly with dietary nitrate (p = 0.004), 1.7-5.1 μM at SL and 1.6-6.3 μM at D5, and this rise appeared to be associated with increased levels of ENO. However, no significant changes occurred to levels of EBC nitrate or nitrosation products (RXNO). Median salivary nitrite/nitrate concentrations increased from 56.5/786 μM to 333/5,194 μM with nitrate supplementation at SL, and changed to 85.6/641 μM and 341/4,553 μM on D5. Salivary RXNO rose markedly with treatment at SL from 0.55 μM to 5.70 μM. At D5 placebo salivary RXNO had increased to 1.90 μM whilst treatment RXNO decreased to 3.26 μM. There was no association with changes in any observation variables or AMS score. In conclusion, dietary nitrate supplementation is well tolerated at altitude and significantly increases pulmonary NO availability and both salivary and EBC NO metabolite concentrations. Surprisingly, this is not associated with changes in hemodynamics, oxygen saturation or AMS development.
Keywords: Altitude; Hypoxaemia; Hypoxia; Nitrate; Nitric oxide; Nitrite.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Grocott M.P.W., Martin D.S., Levett D.Z.H., McMorrow R., Windsor J., Montgomery H.E. Arterial blood gases and oxygen content in climbers on Mount Everest. N. Engl. J. Med. 2009 Jan 8;360(2):140–149. - PubMed
-
- Cumpstey A., Grocott M. High altitude respiratory physiology and pathophysiology. Shortness Breath. 2015;4(3):100–106.
-
- Gilbert-Kawai E.T., Milledge J.S., Grocott M.P.W., Martin D.S. King of the mountains: tibetan and sherpa physiological adaptations for life at high altitude. Physiology. 2014 Nov 1;29(6):388–402. - PubMed
-
- Beall C.M., Laskowski D., Strohl K.P., Soria R., Villena M., Vargas E. Pulmonary nitric oxide in mountain dwellers. Nature. 2001 Nov 22;414(6862):411–412. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
