

Peripheral Artery Disease and Transcatheter Aortic Valve Replacement Outcomes: A Report From the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Therapy Registry
- PMID: 29042398
- PMCID: PMC5683430
- DOI: 10.1161/CIRCINTERVENTIONS.117.005456
Peripheral Artery Disease and Transcatheter Aortic Valve Replacement Outcomes: A Report From the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Therapy Registry
Abstract
Background: Peripheral artery disease (PAD) is associated with increased cardiovascular mortality, and PAD risk factors overlap with those for aortic stenosis. The prevalence and outcomes associated with PAD in a population undergoing transcatheter aortic valve replacement (TAVR) are unknown.
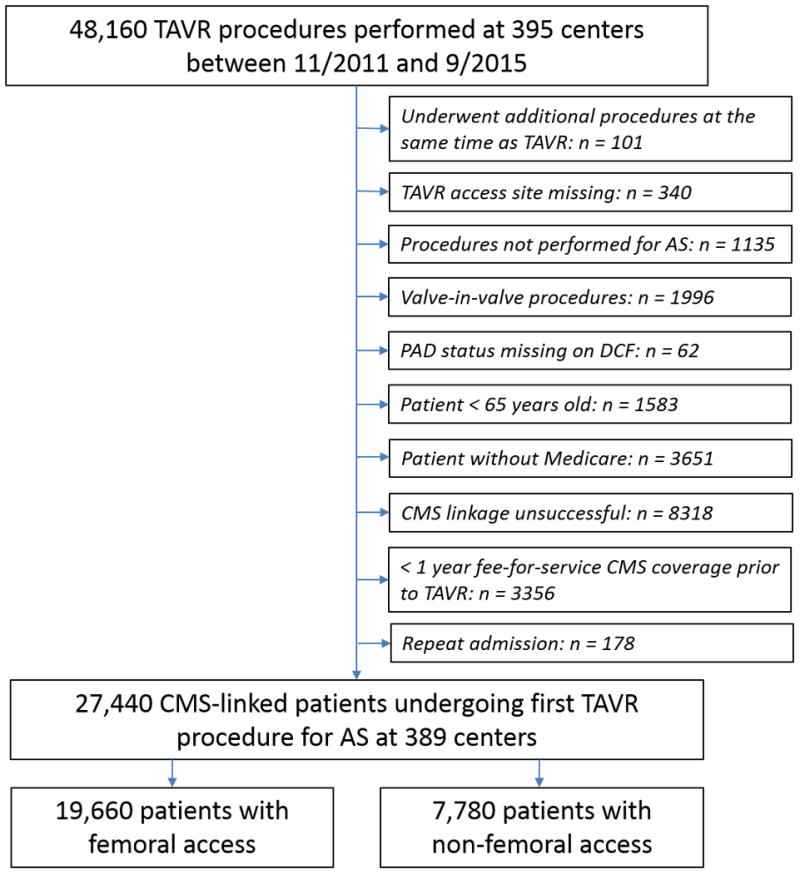
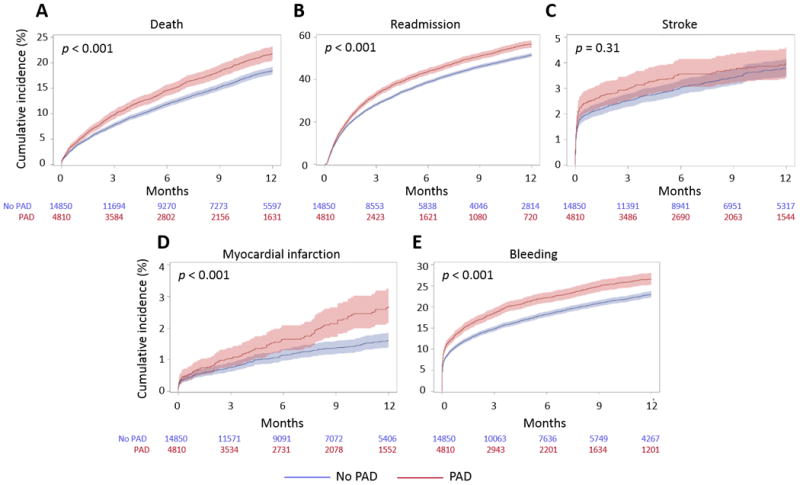
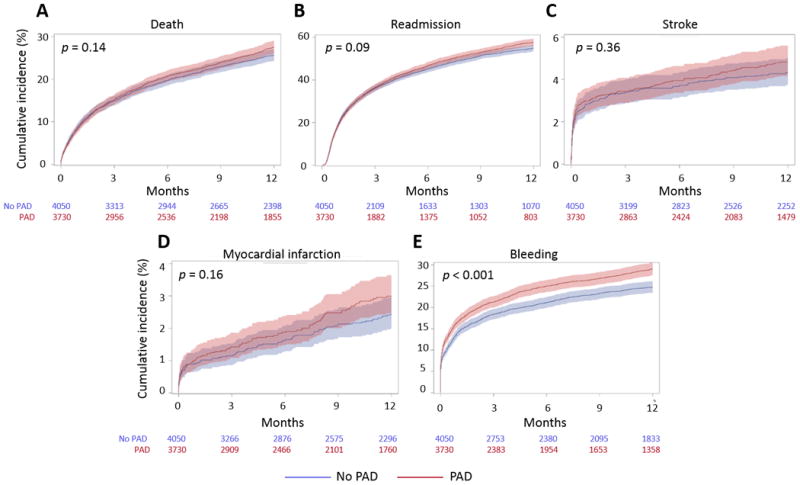
Methods and results: Using the Society of Thoracic Surgeons/Transcatheter Valve Therapy Registry linked to Medicare claims data, we identified patients ≥65 years old undergoing TAVR from 2011 to 2015. We calculated hazard ratios for 1-year adverse outcomes, including mortality, readmission, and bleeding, for patients with PAD compared with those without, adjusting for baseline characteristics and postprocedure medications. Analyses were performed separately by access site (transfemoral and nontransfemoral). Of 19 660 patients undergoing transfemoral TAVR, 4810 (24.5%) had PAD; 3730 (47.9%) of 7780 patients undergoing nontransfemoral TAVR had PAD. In both groups, patients with PAD were significantly more likely to have coronary and carotid artery diseases. At 1-year follow-up, patients with PAD undergoing TAVR via transfemoral access had a higher incidence of death (16.8% versus 14.4%; adjusted hazard ratio, 1.14; P=0.01), readmission (45.5% versus 42.1%; hazard ratio, 1.11; P<0.001), and bleeding (23.1% versus 19.7%; hazard ratio, 1.18; P<0.001) compared with patients without PAD. Patients with PAD undergoing TAVR via nontransfemoral access did not have significantly higher rates of 1-year mortality or readmission compared with patients without PAD.
Conclusions: PAD is common among patients undergoing commercial TAVR via transfemoral and nontransfemoral access. Among patients undergoing transfemoral TAVR, PAD is associated with a higher incidence of 1-year adverse outcomes compared with absence of PAD.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01737528.
Keywords: aortic valve stenosis; peripheral vascular disease; risk factors; transcatheter aortic valve replacement.
© 2017 American Heart Association, Inc.
Figures
References
-
- Fowkes FGR, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–1340. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB. Heart disease and stroke statistics-2015 update: a report from the american heart association. Circulation. 2015;131:e29–e322. - PubMed
-
- Eveborn GW, Schirmer H, Heggelund G, Lunde P, Rasmussen K. The evolving epidemiology of valvular aortic stenosis. the Tromsø study. Heart. 2013;99:396–400. - PubMed
-
- Fusini L, Mirea O, Tamborini G, Muratori M, Gripari P, Cefalù C, Ali SG, Maffessanti F, Andreini D, Pontone G. Incidence and severity of atherosclerotic cardiovascular artery disease in patients undergoing TAVI. Int J Cardiovasc Imaging. 2015;31:975–985. - PubMed
-
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607. - PubMed
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
