

Cardiac Resynchronization Therapy Using Quadripolar Versus Non-Quadripolar Left Ventricular Leads Programmed to Biventricular Pacing With Single-Site Left Ventricular Pacing: Impact on Survival and Heart Failure Hospitalization
- PMID: 29042422
- PMCID: PMC5721885
- DOI: 10.1161/JAHA.117.007026
Cardiac Resynchronization Therapy Using Quadripolar Versus Non-Quadripolar Left Ventricular Leads Programmed to Biventricular Pacing With Single-Site Left Ventricular Pacing: Impact on Survival and Heart Failure Hospitalization
Abstract
Background: In cardiac resynchronization therapy (CRT), quadripolar (QUAD) left ventricular (LV) leads are less prone to postoperative complications than non-QUAD leads. Some studies have suggested better clinical outcomes.
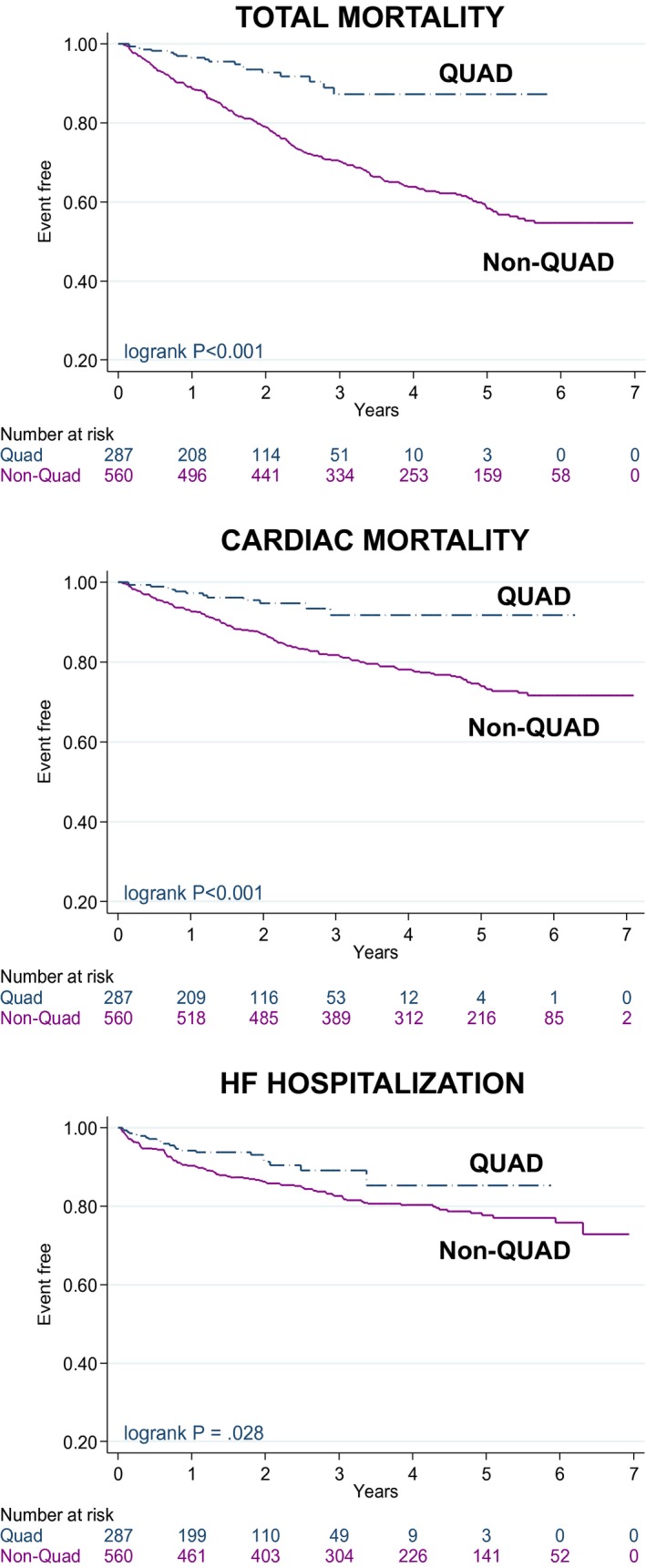
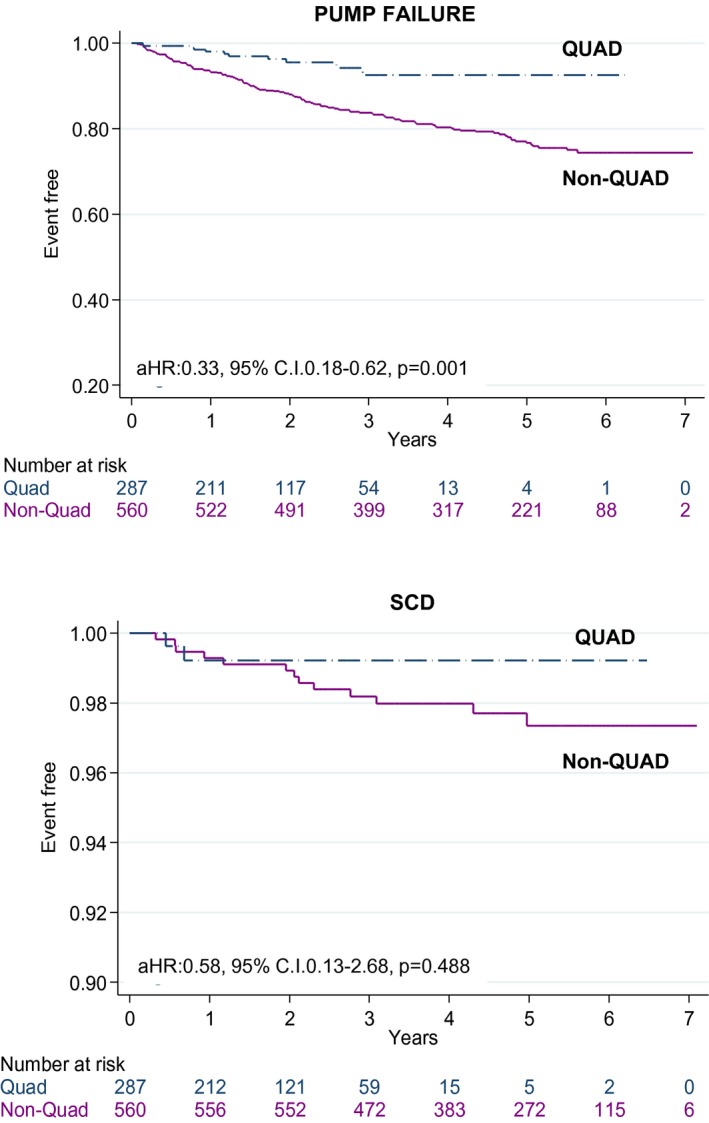
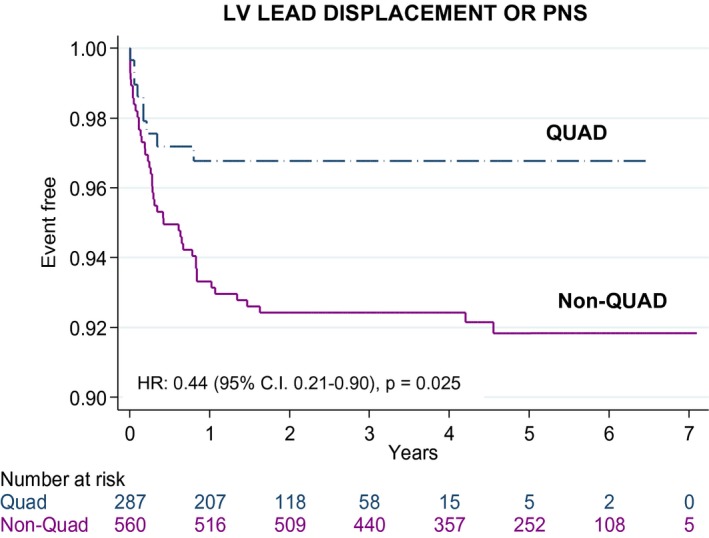
Methods and results: Clinical events were assessed in 847 patients after CRT-pacing or CRT-defibrillation using either QUAD (n=287) or non-QUAD (n=560), programmed to single-site site LV pacing. Over a follow-up period of 3.2 years (median [interquartile range, 1.90-5.0]), QUAD was associated with a lower total mortality (adjusted hazard ratio [aHR]: 0.32, 95% confidence interval [CI], 0.20-0.52), cardiac mortality (aHR: 0.36, 95% CI, 0.20-0.65), and heart failure (HF) hospitalization (aHR: 0.62, 95% CI, 0.39-0.99), after adjustment for age, sex, New York Heart Association class, HF etiology, device type (CRT-pacing or CRT-defibrillation), comorbidities, atrial rhythm, medication, left ventricular ejection fraction, and creatinine. Death from pump failure was lower with QUAD (aHR: 0.33; 95% CI, 0.18-0.62), but no group differences emerged with respect to sudden cardiac death. There were no differences in implant-related complications. Re-interventions for LV displacement or phrenic nerve stimulation, which were lower with QUAD, predicted total mortality (aHR: 1.68, 95% CI, 1.11-2.54), cardiac mortality (aHR: 2.61, 95% CI, 1.66-4.11) and HF hospitalization (aHR: 2.09, 95% CI, 1.22-3.58).
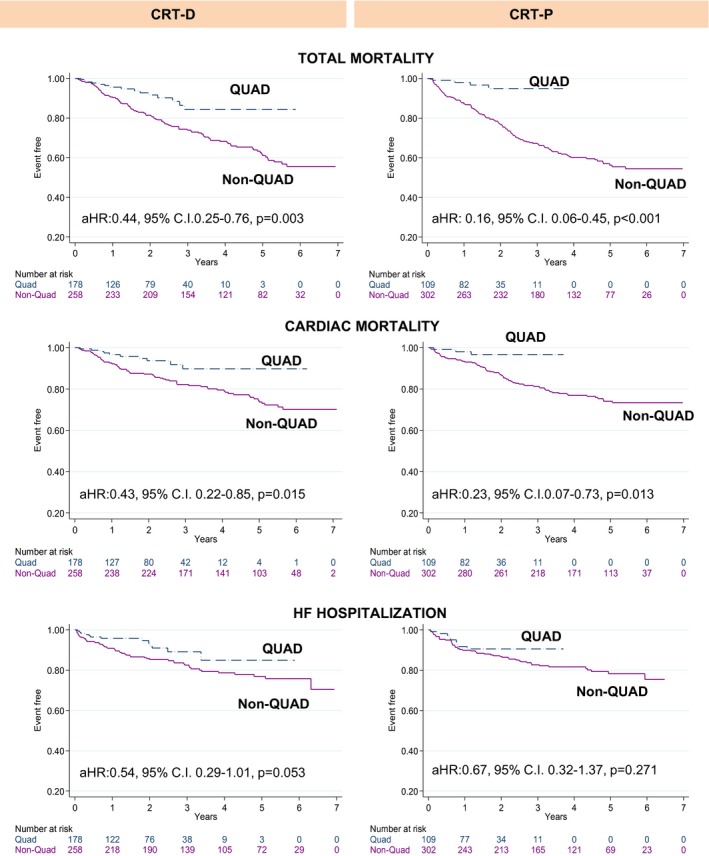
Conclusions: CRT using QUAD, programmed to biventricular pacing with single-site LV pacing, is associated with a lower total mortality, cardiac mortality, and HF hospitalization. These trends were observed for both CRT-defibrillation and CRT-pacing, after adjustment for HF cause and other confounders. Re-intervention for LV lead displacement or phrenic nerve stimulation was associated with worse outcomes.
Keywords: arrhythmia; bipolar lead; cardiac resynchronization therapy; heart failure; quadripolar lead; sudden cardiac death.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Clinical outcome of left ventricular multipoint pacing versus conventional biventricular pacing in cardiac resynchronization therapy: a systematic review and meta-analysis.Heart Fail Rev. 2018 Nov;23(6):927-934. doi: 10.1007/s10741-018-9737-5. Heart Fail Rev. 2018. PMID: 30209643
-
Cardiac Resynchronization Therapy Delivered Via a Multipolar Left Ventricular Lead is Associated with Reduced Mortality and Elimination of Phrenic Nerve Stimulation: Long-Term Follow-Up from a Multicenter Registry.J Cardiovasc Electrophysiol. 2015 May;26(5):540-6. doi: 10.1111/jce.12625. Epub 2015 Mar 5. J Cardiovasc Electrophysiol. 2015. PMID: 25631303 Free PMC article.
-
Impact of quadripolar LV leads on heart failure hospitalization rates among patients implanted with CRT-D: data from the Israeli ICD Registry.J Interv Card Electrophysiol. 2018 Jan;51(1):5-12. doi: 10.1007/s10840-017-0305-z. Epub 2017 Dec 23. J Interv Card Electrophysiol. 2018. PMID: 29274032
-
Sex Differences in Long-Term Outcomes With Cardiac Resynchronization Therapy in Mild Heart Failure Patients With Left Bundle Branch Block.J Am Heart Assoc. 2015 Jun 29;4(7):e002013. doi: 10.1161/JAHA.115.002013. J Am Heart Assoc. 2015. PMID: 26124205 Free PMC article. Clinical Trial.
-
Right ventricular lead location and outcomes among patients with cardiac resynchronization therapy: A meta-analysis.Prog Cardiovasc Dis. 2021 May-Jun;66:53-60. doi: 10.1016/j.pcad.2021.04.002. Epub 2021 Apr 20. Prog Cardiovasc Dis. 2021. PMID: 33864874 Free PMC article.
Cited by
-
Scar burden is an independent and incremental predictor of cardiac resynchronisation therapy response.Open Heart. 2019 Jul 5;6(2):e001067. doi: 10.1136/openhrt-2019-001067. eCollection 2019. Open Heart. 2019. PMID: 31354957 Free PMC article.
-
Performance of an active fixation bipolar left ventricular lead vs passive fixation quadripolar leads in cardiac resynchronization therapy, a randomized trial.J Arrhythm. 2020 Nov 8;37(1):212-218. doi: 10.1002/joa3.12450. eCollection 2021 Feb. J Arrhythm. 2020. PMID: 33664905 Free PMC article.
-
Comment on 'Leadless Pacemakers: Current Achievements and Future Perspectives'.Eur Cardiol. 2023 Aug 18;18:e50. doi: 10.15420/ecr.2022.58. eCollection 2023. Eur Cardiol. 2023. PMID: 37655135 Free PMC article. No abstract available.
-
Improved prognosis after cardiac resynchronization therapy over a decade.Europace. 2023 Jun 2;25(6):euad141. doi: 10.1093/europace/euad141. Europace. 2023. PMID: 37265253 Free PMC article.
-
Clinical outcome of left ventricular multipoint pacing versus conventional biventricular pacing in cardiac resynchronization therapy: a systematic review and meta-analysis.Heart Fail Rev. 2018 Nov;23(6):927-934. doi: 10.1007/s10741-018-9737-5. Heart Fail Rev. 2018. PMID: 30209643
References
-
- Leyva F, Nisam S, Auricchio A. 20 years of cardiac resynchronization therapy. J Am Coll Cardiol. 2014;64:1047–1058. - PubMed
-
- Daubert JC, Ritter P, Le Breton H, Gras D, Leclercq C, Lazarus A, Mugica J, Mabo P, Cazeau S. Permanent left ventricular pacing with transvenous leads inserted into the coronary veins. Pacing Clin Electrophysiol. 1998;21:239–245. - PubMed
-
- Auricchio A, Klein H, Tockman B, Sack S, Stellbrink C, Neuzner J, Kramer A, Ding J, Pochet T, Maarse A, Spinelli J. Transvenous biventricular pacing for heart failure: can the obstacles be overcome? Am J Cardiol. 1999;83:136D–142D. - PubMed
-
- Sperzel J, Danschel W, Gutleben KJ, Kranig W, Mortensen P, Connelly D, Trappe HJ, Seidl K, Duray G, Pieske B, Stockinger J, Boriani G, Jung W, Schilling R, Saberi L, Hallier B, Simon M, Rinaldi CA. First prospective, multi‐centre clinical experience with a novel left ventricular quadripolar lead. Europace. 2012;14:365–372. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
