

Effects of Two Immunosuppressive Treatment Protocols for IgA Nephropathy
- PMID: 29042456
- PMCID: PMC5748925
- DOI: 10.1681/ASN.2017060713
Effects of Two Immunosuppressive Treatment Protocols for IgA Nephropathy
Abstract
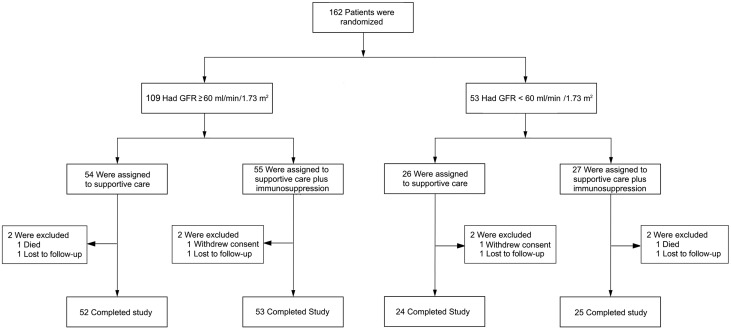
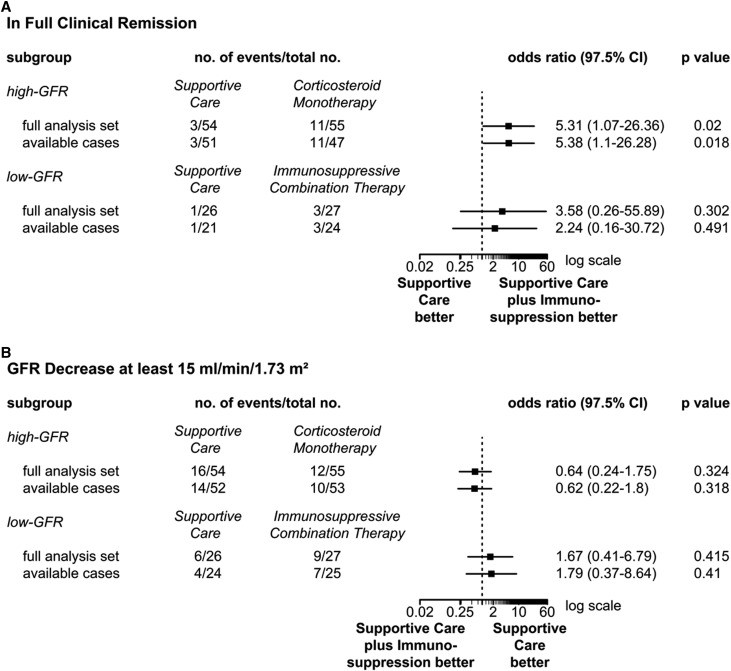
The role of immunosuppression in IgA nephropathy (IgAN) is controversial. In the Supportive Versus Immunosuppressive Therapy for the Treatment of Progressive IgA Nephropathy (STOP-IgAN) Trial, 162 patients with IgAN and proteinuria >0.75 g/d after 6 months of optimized supportive care were randomized into two groups: continued supportive care or additional immunosuppression (GFR≥60 ml/min per 1.73 m2: 6-month corticosteroid monotherapy; GFR=30-59 ml/min per 1.73 m2: cyclophosphamide for 3 months followed by azathioprine plus oral prednisolone). Coprimary end points were full clinical remission and GFR loss ≥15 ml/min per 1.73 m2 during the 3-year trial phase. In this secondary intention to treat analysis, we separately analyzed data from each immunosuppression subgroup and the corresponding patients on supportive care. Full clinical remission occurred in 11 (20%) patients receiving corticosteroid monotherapy and three (6%) patients on supportive care (odds ratio, 5.31; 95% confidence interval, 1.07 to 26.36; P=0.02), but the rate did not differ between patients receiving immunosuppressive combination and controls on supportive care (11% versus 4%, respectively; P=0.30). The end point of GFR loss ≥15 ml/min per 1.73 m2 did not differ between groups. Only corticosteroid monotherapy transiently reduced proteinuria at 12 months. Severe infections, impaired glucose tolerance, and/or weight gain in the first year were more frequent with either immunosuppressive regimen than with supportive care. In conclusion, only corticosteroid monotherapy induced disease remission in a minority of patients who had IgAN with relatively well preserved GFR and persistent proteinuria. Neither immunosuppressive regimen prevented GFR loss, and both associated with substantial adverse events.
Keywords: IgA nephropathy; glomerular disease; glomerulonephritis; immunosuppression.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- KDIGO: KDIGO clinical practice guideline for glomerulonephritis. Kidney Int Suppl (2011) 2: 139–274, 2012
-
- Pozzi C, Bolasco PG, Fogazzi GB, Andrulli S, Altieri P, Ponticelli C, Locatelli F: Corticosteroids in IgA nephropathy: A randomised controlled trial. Lancet 353: 883–887, 1999 - PubMed
-
- Pozzi C, Andrulli S, Del Vecchio L, Melis P, Fogazzi GB, Altieri P, Ponticelli C, Locatelli F: Corticosteroid effectiveness in IgA nephropathy: Long-term results of a randomized, controlled trial. J Am Soc Nephrol 15: 157–163, 2004 - PubMed
-
- Manno C, Torres DD, Rossini M, Pesce F, Schena FP: Randomized controlled clinical trial of corticosteroids plus ACE-inhibitors with long-term follow-up in proteinuric IgA nephropathy. Nephrol Dial Transplant 24: 3694–3701, 2009 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
