

Hypereosinophilia Secondary to Disseminated Paracoccidioidomycosis
- PMID: 29042530
- PMCID: PMC5659236
- DOI: 10.12659/ajcr.904520
Hypereosinophilia Secondary to Disseminated Paracoccidioidomycosis
Abstract
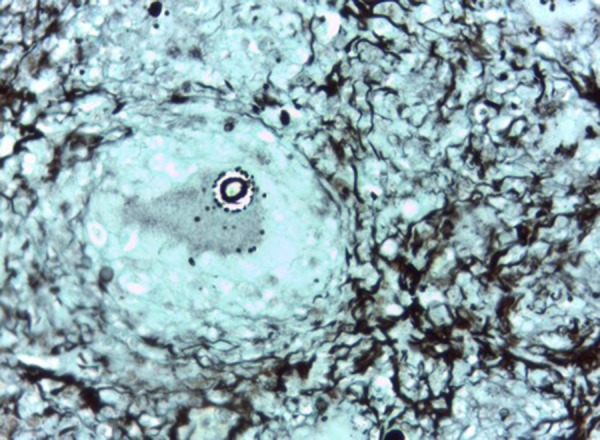
BACKGROUND Paracoccidioidomycosis is an endemic mycosis in Central and South America caused by the thermally dimorphic fungus Paracoccidioides brasiliensis. Despite its self-limited course and usually asymptomatic infection, some patients may present with a systemic illness mimicking multiple conditions and thus question the general state of their immune system. CASE REPORT A 28-year-old male presented to the hospital with fever, dry cough, and non-pruritic rash with no characteristic distribution for the past 10 days. Past medical history revealed that the patient had worked as a farmer three years ago, had abused cocaine paste over the same period, and also had in the last month presented to the hospital for acute appendicitis. Initial laboratory tests revealed hypereosinophilia greater than 10,000 eosinophils/mL. Infection of P. brasiliensis was confirmed by lymph node, skin, and colonoscopy biopsies. After treatment with itraconazole, the patient's eosinophil count returned to normal and his symptoms resolved. CONCLUSIONS Paracoccidioidomycosis may present as a systemic illness with only marked eosinophilia on initial diagnostic tests. Furthermore, in our patient's case, the high degree of eosinophilia may have contributed towards the patient's appendicitis in the weeks preceding the subacute infection. It is possible that the patient's history of working at a farm and abusing cocaine paste may have contributed to the initial colonization by the fungus.
Conflict of interest statement
Figures

Similar articles
-
A case of imported paracoccidioidomycosis: an awkward infection in The Netherlands.Med Mycol. 2006 Feb;44(1):13-8. doi: 10.1080/13693780500148137. Med Mycol. 2006. PMID: 16805088
-
Primary complex of paracoccidioidomycosis and hypereosinophilia.J Bras Pneumol. 2009 Dec;35(12):1259-62. doi: 10.1590/s1806-37132009001200016. J Bras Pneumol. 2009. PMID: 20126931 English, Portuguese.
-
[Paracoccidioidomycosis in pediatric patients: a description of 4 cases].Rev Iberoam Micol. 2014 Apr-Jun;31(2):141-4. doi: 10.1016/j.riam.2013.05.013. Epub 2013 Jun 20. Rev Iberoam Micol. 2014. PMID: 23792123 Spanish.
-
Pulmonary paracoccidioidomycosis.Semin Respir Crit Care Med. 2011 Dec;32(6):764-74. doi: 10.1055/s-0031-1295724. Epub 2011 Dec 13. Semin Respir Crit Care Med. 2011. PMID: 22167404 Review.
-
Chapter 6--paracoccidioidomycosis.J Bras Pneumol. 2009 Dec;35(12):1245-9. doi: 10.1590/s1806-37132009001200013. J Bras Pneumol. 2009. PMID: 20126928 Review. English, Portuguese.
Cited by
-
Intestinal Paracoccidioidomycosis: Case report and literature review.Int J Surg Case Rep. 2022 Feb;91:106801. doi: 10.1016/j.ijscr.2022.106801. Epub 2022 Jan 29. Int J Surg Case Rep. 2022. PMID: 35121286 Free PMC article.
References
-
- Restrepo A, Gómez BL, Tobón A. Paracoccidioidomycosis: Latin America’s own fungal disorder. Curr Fungal Infect Rep. 2012;6(4):303–11.
-
- Morejón KML, Machado AA, Martinez R. Paracoccidioidomycosis in patients infected with and not infected with human immunodeficiency virus: A case-control study. Am J Trop Med Hyg. 2009;80(3):359–66. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
