

Asthma symptoms, mannitol reactivity and exercise-induced bronchoconstriction in adolescent swimmers versus tennis players
- PMID: 29042799
- PMCID: PMC5633302
- DOI: 10.2147/JAA.S134794
Asthma symptoms, mannitol reactivity and exercise-induced bronchoconstriction in adolescent swimmers versus tennis players
Abstract
Background: Strenuous physical activity at an elite level is associated with an increased risk for asthma and, in some sports, also prevalence of allergies. The aim of this study was to investigate the prevalence of asthma and allergy among elite swimmers and tennis players and compare airway hyperreactivity to mannitol and exercise.
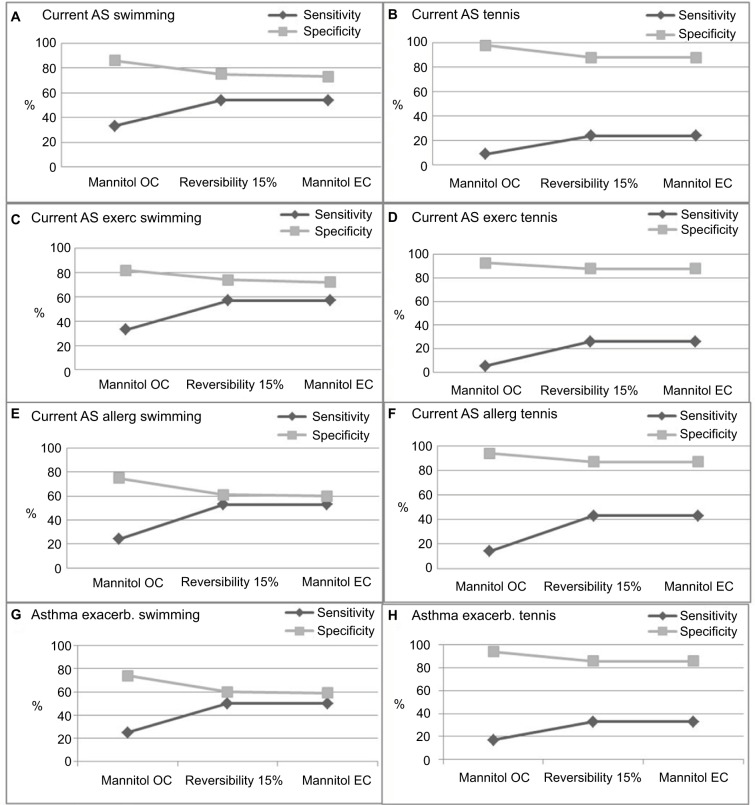
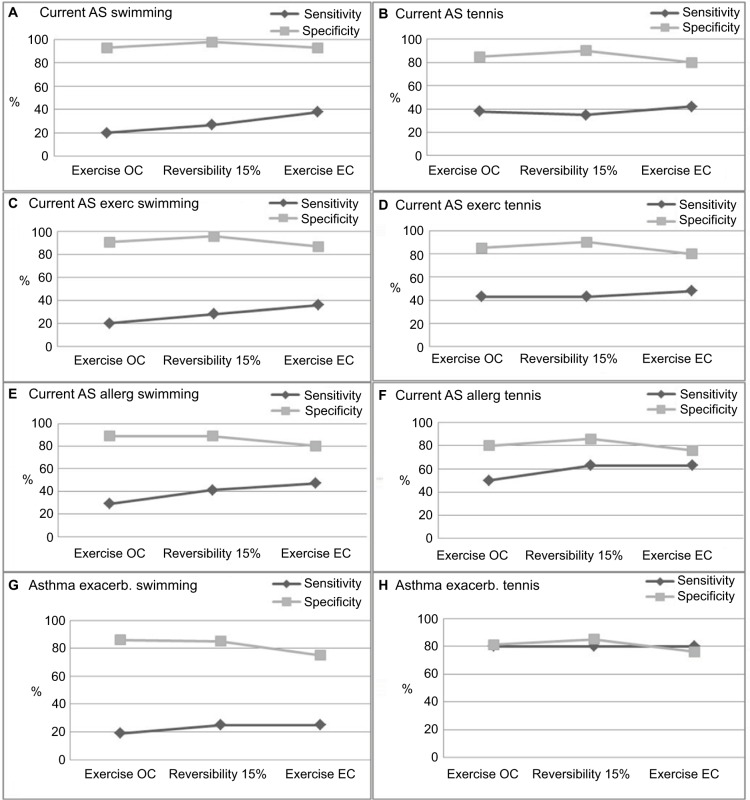
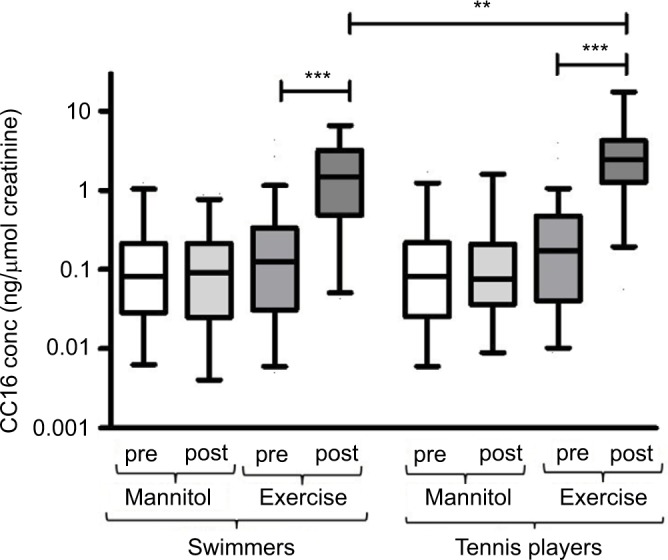
Materials and methods: One hundred and one adolescent swimmers and 86 tennis players answered a questionnaire about respiratory symptoms and allergy and performed mannitol challenge and sport-specific exercise challenge. Atopy was assessed and fractional exhaled nitric oxide was measured. Mannitol positivity was defined as drop in FEV1 ≥15% (ordinary criteria) and/or β2-reversibility (≥15%) after provocation (extended criteria). A positive exercise test was defined as a drop in FEV1 ≥10% (ordinary criteria) and/or β2-reversibility (≥15%) after provocation (extended criteria). Club cell protein (CC16) was measured in urine before and after the challenges.
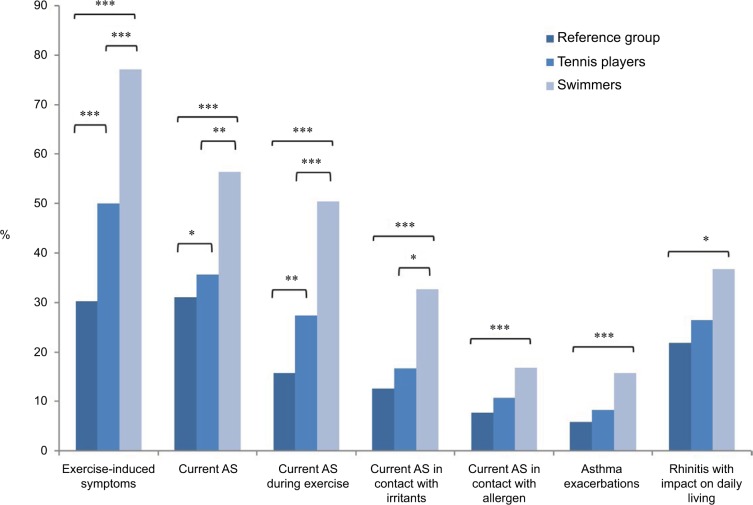
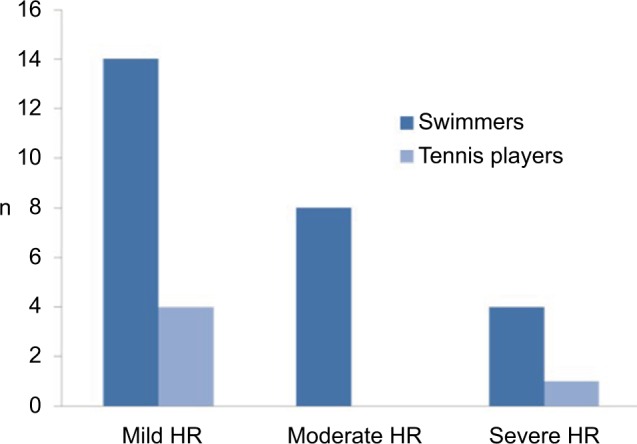
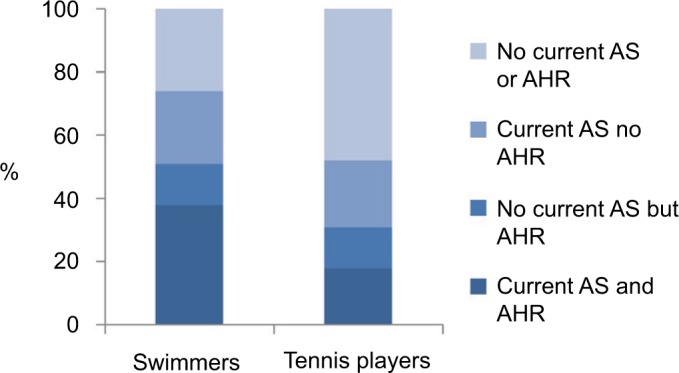
Results: Asthma symptoms were common in both groups. More swimmers had exercise-induced symptoms (77% versus 50%) and current asthma symptoms (56% versus 38%), compared to the tennis players. More swimmers also had a positive mannitol challenge test both using ordinary (26% versus 6%) and extended criteria (43% versus 17%), while the number of positive exercise tests did not differ. After exercise (but not mannitol) challenge, CC16 level was increased in both groups, but to a higher extent in tennis players. There were no differences in atopy, rhinitis or fractional exhaled nitric oxide.
Conclusion: We found a high prevalence of asthma among elite swimmers and tennis players and a higher frequency of current asthma and positive mannitol challenge tests among the swimmers. This indicates an unfavorable exercise environment.
Keywords: CC16 bronchial hyperreactivity; asthma; bronchial hyperreactivity test; exercise; mannitol; sport; swimming; tennis.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Extended diagnostic criteria used for indirect challenge testing in elite asthmatic swimmers.Respir Med. 2012 Jan;106(1):15-24. doi: 10.1016/j.rmed.2011.09.011. Epub 2011 Oct 27. Respir Med. 2012. PMID: 22035852
-
Sex differences in asthma in swimmers and tennis players.Ann Allergy Asthma Immunol. 2017 Mar;118(3):311-317. doi: 10.1016/j.anai.2016.12.013. Epub 2017 Jan 23. Ann Allergy Asthma Immunol. 2017. PMID: 28126431
-
Exercise but not mannitol provocation increases urinary Clara cell protein (CC16) in elite swimmers.Respir Med. 2011 Jan;105(1):31-6. doi: 10.1016/j.rmed.2010.07.012. Epub 2010 Aug 8. Respir Med. 2011. PMID: 20696561
-
Allergy and asthma in elite summer sport athletes.J Allergy Clin Immunol. 2000 Sep;106(3):444-52. doi: 10.1067/mai.2000.107749. J Allergy Clin Immunol. 2000. PMID: 10984362 Review.
-
Exercise and other indirect challenges to demonstrate asthma or exercise-induced bronchoconstriction in athletes.J Allergy Clin Immunol. 2008 Aug;122(2):238-46; quiz 247-8. doi: 10.1016/j.jaci.2008.06.014. J Allergy Clin Immunol. 2008. PMID: 18678339 Review.
Cited by
-
Asthma, allergies and respiratory symptoms in different activity groups of swimmers exercising in swimming halls.BMC Sports Sci Med Rehabil. 2021 Oct 4;13(1):119. doi: 10.1186/s13102-021-00349-2. BMC Sports Sci Med Rehabil. 2021. PMID: 34607605 Free PMC article.
-
Equine Asthma Diagnostics: Review of Influencing Factors and Difficulties in Diagnosing Subclinical Disease.Animals (Basel). 2024 Dec 4;14(23):3504. doi: 10.3390/ani14233504. Animals (Basel). 2024. PMID: 39682469 Free PMC article. Review.
-
The Prevalence of Asthma and Respiratory Symptoms among Cross-Country Skiers in Early Adolescence.Can Respir J. 2019 Sep 15;2019:1514353. doi: 10.1155/2019/1514353. eCollection 2019. Can Respir J. 2019. PMID: 31636769 Free PMC article.
-
Influence of exercise duration on respiratory function and systemic immunity among healthy, endurance-trained participants exercising in sub-zero conditions.Respir Res. 2022 May 12;23(1):121. doi: 10.1186/s12931-022-02029-2. Respir Res. 2022. PMID: 35550109 Free PMC article. Clinical Trial.
-
Studying Respiratory Symptoms Related to Swimming Pools Attendance in Young Athletes: The SPHeRA Study.Toxics. 2022 Dec 6;10(12):759. doi: 10.3390/toxics10120759. Toxics. 2022. PMID: 36548592 Free PMC article.
References
-
- American Thoracic Society; European Respiratory Society ATS/ERS recommendations for standardized procedures for online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide. Am J Respir Crit Care Med. 2005;171(8):912–930. - PubMed
-
- Anderson SD, Brannan JD. Methods for “indirect” challenge tests including exercise, eucapnic voluntary hyperpnea, and hypertonic aerosols. Clin Rev Allergy Immunol. 2003;24(1):27–54. - PubMed
-
- Randolph CC. Allergic rhinitis and asthma in the athlete. Allergy Asthma Proc. 2006;27(2):104–109. - PubMed
-
- Carlsen KH, Anderson SD, Bjermer L, et al. Exercise-induced asthma, respiratory and allergic disorders in elite athletes: epidemiology, mechanisms and diagnosis: part I of the report from the Joint Task Force of the European Respiratory Society (ERS) and the European Academy of Allergy and Clinical Immunology (EAACI) in cooperation with GA2LEN. Allergy. 2008;63(4):387–403. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
