

Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting
- PMID: 29043428
- PMCID: PMC5834554
- DOI: 10.1007/s00330-017-5026-2
Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting
Erratum in
-
Correction to: Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting.Eur Radiol. 2018 Jun;28(6):2711. doi: 10.1007/s00330-017-5204-2. Eur Radiol. 2018. PMID: 29322331 Free PMC article.
Abstract
Objectives: To update the 2012 ESGAR consensus guidelines on the acquisition, interpretation and reporting of magnetic resonance imaging (MRI) for clinical staging and restaging of rectal cancer.
Methods: Fourteen abdominal imaging experts from the European Society of Gastrointestinal and Abdominal Radiology (ESGAR) participated in a consensus meeting, organised according to an adaptation of the RAND-UCLA Appropriateness Method. Two independent (non-voting) Chairs facilitated the meeting. 246 items were scored (comprising 229 items from the previous 2012 consensus and 17 additional items) and classified as 'appropriate' or 'inappropriate' (defined by ≥ 80 % consensus) or uncertain (defined by < 80 % consensus).
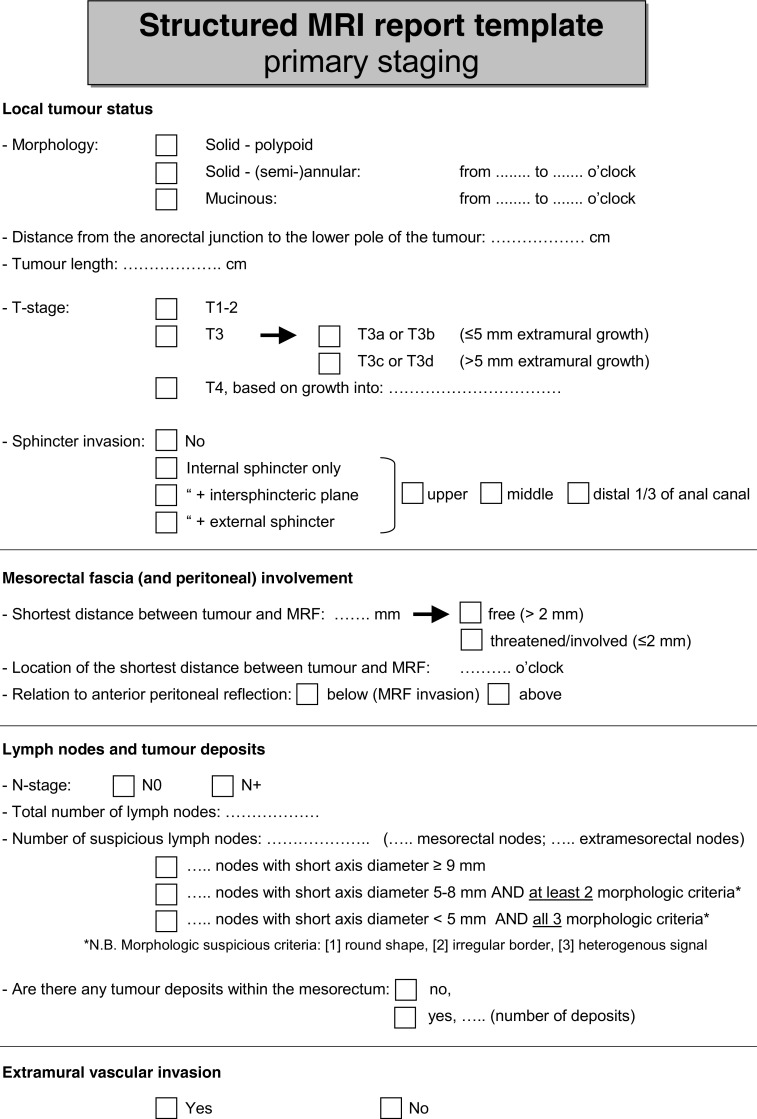
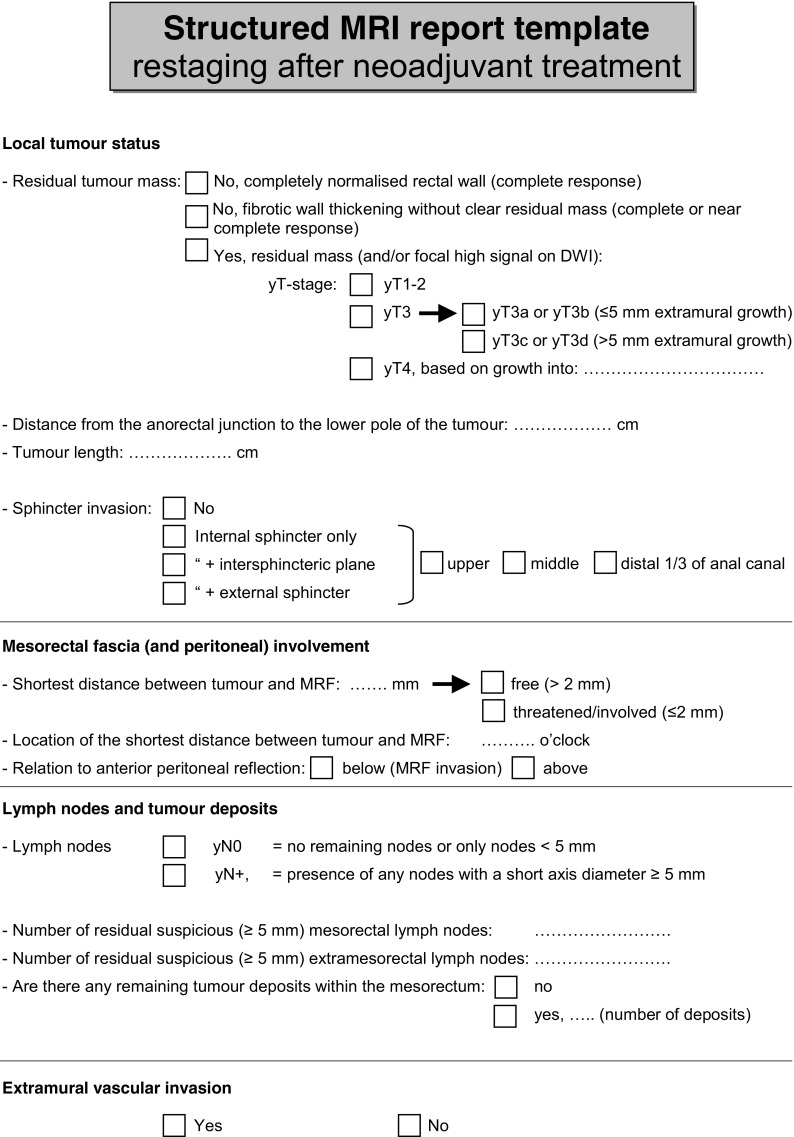
Results: Consensus was reached for 226 (92 %) of items. From these recommendations regarding hardware, patient preparation, imaging sequences and acquisition, criteria for MR imaging evaluation and reporting structure were constructed. The main additions to the 2012 consensus include recommendations regarding use of diffusion-weighted imaging, criteria for nodal staging and a recommended structured report template.
Conclusions: These updated expert consensus recommendations should be used as clinical guidelines for primary staging and restaging of rectal cancer using MRI.
Key points: • These guidelines present recommendations for staging and reporting of rectal cancer. • The guidelines were constructed through consensus amongst 14 pelvic imaging experts. • Consensus was reached by the experts for 92 % of the 246 items discussed. • Practical guidelines for nodal staging are proposed. • A structured reporting template is presented.
Keywords: Cancer rectal neoplasms; Magnetic resonance imaging; Staging; Standards; Structured reporting.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is D. Lambregts.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
S. Bipat kindly provided statistical advice for this manuscript.
Informed consent
The study concerns a consensus paper and therefore no patients were involved. Institutional review board permission is not applicable.
Ethical approval
Institutional Review Board approval was not required because the study is based on a consensus meeting and no patients were involved.
Study subjects or cohorts overlap
The study presents an update of the previously published consensus meeting from 2012 (Eur Radiol 2013; 23: 2522-2231).
Methodology
• Not applicable
• Not applicable
• Multicentre study
Figures
References
-
- Beets-Tan RG, Lambregts DM, Maas M, et al. Magnetic resonance imaging for the clinical management of rectal cancer patients: recommendations from the 2012 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2013;23:2522–2531. doi: 10.1007/s00330-013-2864-4. - DOI - PubMed
-
- Habr-Gama A, Gama-Rodrigues J, Sao Juliao GP, et al. Local recurrence after complete clinical response and watch and wait in rectal cancer after neoadjuvant chemoradiation: impact of salvage therapy on local disease control. Int J Radiat Oncol Biol Phys. 2014;88:822–828. doi: 10.1016/j.ijrobp.2013.12.012. - DOI - PubMed
-
- Martens MH, Maas M, Heijnen LA, et al (2016) Long-term outcome of an organ preservation program after neoadjuvant treatment for rectal cancer. J Natl Cancer Inst. 108 - PubMed
-
- Fitch K, Bernstein S, Aguilar M, et al. The RAND/UCLA Appropriateness Method User’s Manual. AHCPR Pub No 95-0009. Rockville: Public Health Service, US Department of Health and Human Services; 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
