

Comparison of strain imaging techniques in CRT candidates: CMR tagging, CMR feature tracking and speckle tracking echocardiography
- PMID: 29043465
- PMCID: PMC5847211
- DOI: 10.1007/s10554-017-1253-5
Comparison of strain imaging techniques in CRT candidates: CMR tagging, CMR feature tracking and speckle tracking echocardiography
Abstract
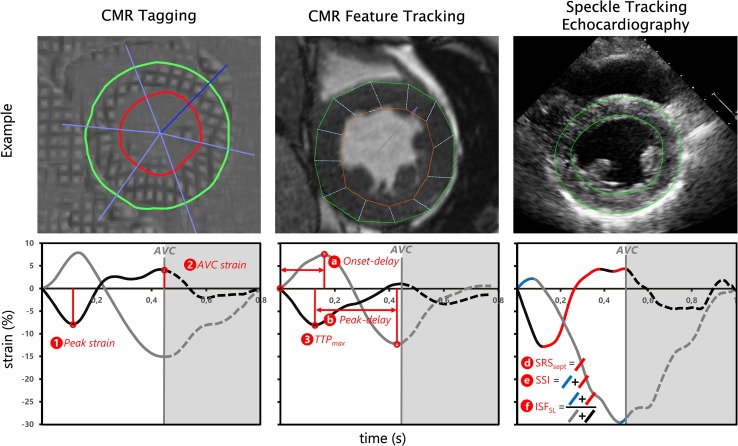
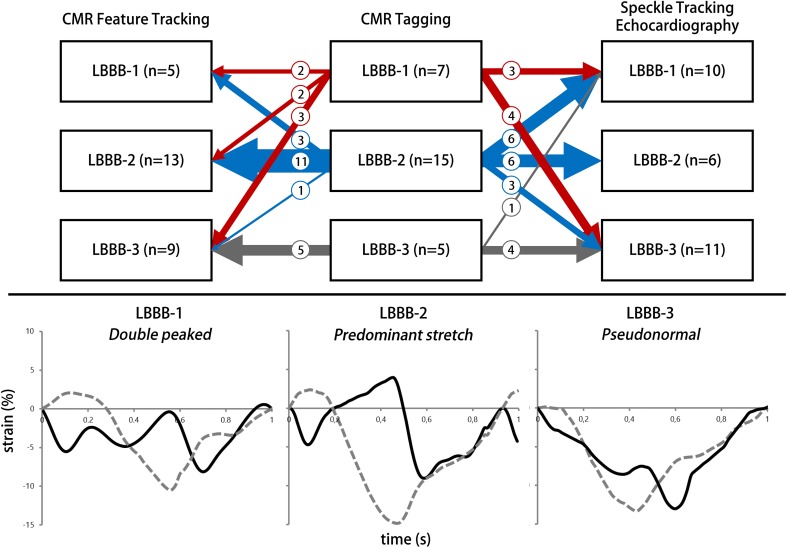
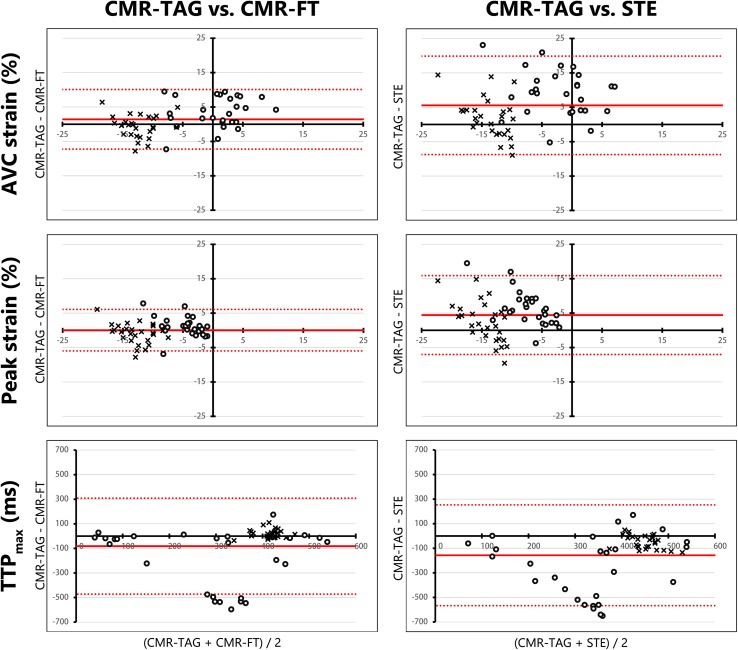
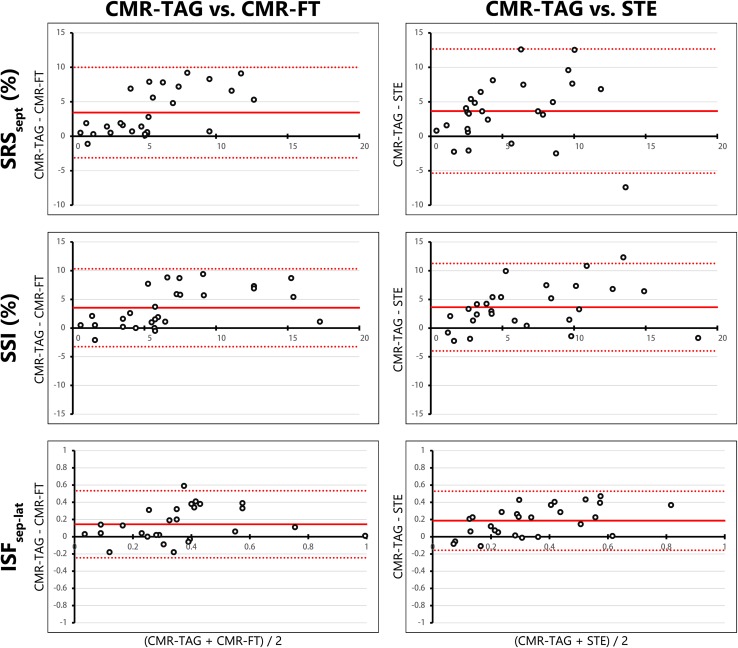
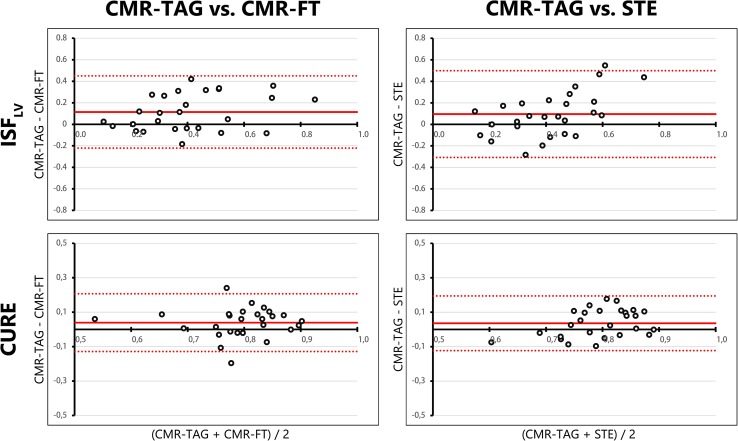
Parameters using myocardial strain analysis may predict response to cardiac resynchronization therapy (CRT). As the agreement between currently available strain imaging modalities is unknown, three different modalities were compared. Twenty-seven CRT-candidates, prospectively included in the MARC study, underwent cardiac magnetic resonance (CMR) imaging and echocardiographic examination. Left ventricular (LV) circumferential strain was analysed with CMR tagging (CMR-TAG), CMR feature tracking (CMR-FT), and speckle tracking echocardiography (STE). Basic strain values and parameters of dyssynchrony and discoordination obtained with CMR-FT and STE were compared to CMR-TAG. Agreement of CMR-FT and CMR-TAG was overall fair, while agreement between STE and CMR-TAG was often poor. For both comparisons, agreement on discoordination parameters was highest, followed by dyssynchrony and basic strain parameters. For discoordination parameters, agreement on systolic stretch index was highest, with fair intra-class correlation coefficients (ICC) (CMR-FT: 0.58, STE: 0.55). ICC of septal systolic rebound stretch (SRSsept) was poor (CMR-FT: 0.41, STE: 0.30). Internal stretch factor of septal and lateral wall (ISFsep-lat) showed fair ICC values (CMR-FT: 0.53, STE: 0.46), while the ICC of the total LV (ISFLV) was fair for CMR-FT (0.55) and poor for STE (ICC: 0.32). The CURE index had a fair ICC for both comparisons (CMR-FT: 0.49, STE 0.41). Although comparison of STE to CMR-TAG was limited by methodological differences, agreement between CMR-FT and CMR-TAG was overall higher compared to STE and CMR-TAG. CMR-FT is a potential clinical alternative for CMR-TAG and STE, especially in the detection of discoordination in CRT-candidates.
Keywords: Cardiac resynchronization therapy; Discoordination; Dyssynchrony; Feature tracking; Myocardial tagging; Speckle tracking echocardiography; Strain.
Conflict of interest statement
Conflict of interests
Wouter M. van Everdingen, Alwin Zweerink, Robin Nijveldt, Odette A.E. Salden, Mathias Meine, Alexander H. Maass, Frederik J. De Lange, Albert C. van Rossum, Pierre Croisille, Patrick Clarysse, Bastiaan Geelhoed, Michiel Rienstra, Isabelle C. Van Gelder, Cornelis P. Allaart, Maarten J. Cramer declare that they have no conflict of interests. Dr. Vernooy received consultancy fee from Medtronic; research grants from Medtronic; speaker fees from St. Jude Medical. Dr. Maass received lecture fees from Medtronic and LivaNova. Dr. Vos received funding from CTMM COHFAR, CVON Predict, EU TrigTreat, EU CERT-ICD and GiLead to perform (pre)clinical studies.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
Similar articles
-
Strain imaging to predict response to cardiac resynchronization therapy: a systematic comparison of strain parameters using multiple imaging techniques.ESC Heart Fail. 2018 Dec;5(6):1130-1140. doi: 10.1002/ehf2.12335. Epub 2018 Jul 26. ESC Heart Fail. 2018. PMID: 30051598 Free PMC article.
-
Comparison of strain parameters in dyssynchronous heart failure between speckle tracking echocardiography vendor systems.Cardiovasc Ultrasound. 2017 Oct 18;15(1):25. doi: 10.1186/s12947-017-0116-5. Cardiovasc Ultrasound. 2017. PMID: 29047378 Free PMC article. Clinical Trial.
-
Left ventricular mechanics assessed by two-dimensional echocardiography and cardiac magnetic resonance imaging: comparison of high-resolution speckle tracking and feature tracking.Eur Heart J Cardiovasc Imaging. 2016 Dec;17(12):1370-1378. doi: 10.1093/ehjci/jew042. Epub 2016 Mar 24. Eur Heart J Cardiovasc Imaging. 2016. PMID: 27013249
-
Assessment of mechanical dyssynchrony in cardiac resynchronization therapy.Dan Med J. 2014 Dec;61(12):B4981. Dan Med J. 2014. PMID: 25441737 Review.
-
Role of speckle tracking echocardiography beyond current guidelines in cardiac resynchronization therapy.Int J Cardiol. 2024 May 1;402:131885. doi: 10.1016/j.ijcard.2024.131885. Epub 2024 Feb 20. Int J Cardiol. 2024. PMID: 38382847 Review.
Cited by
-
Strain imaging to predict response to cardiac resynchronization therapy: a systematic comparison of strain parameters using multiple imaging techniques.ESC Heart Fail. 2018 Dec;5(6):1130-1140. doi: 10.1002/ehf2.12335. Epub 2018 Jul 26. ESC Heart Fail. 2018. PMID: 30051598 Free PMC article.
-
Efficiency is key.Eur Heart J Cardiovasc Imaging. 2020 Feb 1;21(2):154-156. doi: 10.1093/ehjci/jez260. Eur Heart J Cardiovasc Imaging. 2020. PMID: 31630186 Free PMC article. No abstract available.
-
Simultaneous assessment of left ventricular mechanical dyssynchrony using integrated 13N-ammonia PETMR system: direct comparison of PET phase analysis and MR feature tracking.J Nucl Cardiol. 2023 Oct;30(5):1947-1958. doi: 10.1007/s12350-023-03225-3. Epub 2023 Mar 14. J Nucl Cardiol. 2023. PMID: 36918456
-
Evaluation of myocardial strain using cardiovascular magnetic resonance imaging in patients with β-thalassemia major.J Cardiovasc Imaging. 2024 Sep 2;32(1):26. doi: 10.1186/s44348-024-00033-2. J Cardiovasc Imaging. 2024. PMID: 39252137 Free PMC article. No abstract available.
-
CMR in heart failure patients with left bundle branch block: pathophysiology before tissue characterization for better selection of candidates for resynchronisation therapy.Int J Cardiovasc Imaging. 2021 Jul;37(7):2257-2258. doi: 10.1007/s10554-021-02222-2. Epub 2021 Mar 21. Int J Cardiovasc Imaging. 2021. PMID: 33745097 Free PMC article. No abstract available.
References
-
- Daubert JC, Saxon L, Adamson PB, Auricchio A, Berger RD, Beshai JF, et al. 2012 EHRA/HRS expert consensus statement on cardiac resynchronization therapy in heart failure: implant and follow-up recommendations and management. Europace. 2012;14(9):1236–1286. doi: 10.1093/europace/eus222. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
