

Initiation of antihypertensive monotherapy and incident fractures among Medicare beneficiaries
- PMID: 29043521
- PMCID: PMC5645300
- DOI: 10.1186/s40621-017-0125-8
Initiation of antihypertensive monotherapy and incident fractures among Medicare beneficiaries
Abstract
Background: Research suggests antihypertensive medications are associated with fractures in older adults, however results are inconsistent and few have examined how the association varies over time. We sought to examine the association between antihypertensive class and incident non-vertebral fractures among older adults initiating monotherapy according to time since initiation.
Methods: We used a new-user cohort design to identify Medicare beneficiaries (≥ 65 years of age) initiating antihypertensive monotherapy during 2008-2011 using a 20% random sample of Fee-For-Service Medicare beneficiaries enrolled in parts A (inpatient services), B (outpatient services), and D (prescription medication) coverage. Starting the day after the initial antihypertensive prescription, we followed beneficiaries for incident non-vertebral fractures. We used multinomial logistic regression models to estimate propensity scores for initiating each antihypertensive drug class. Using these propensity scores, we weighted beneficiaries to achieve the same baseline covariate distribution as beneficiaries initiating with angiotensin-converting enzyme inhibitors. Lastly, we used weighted Cox proportional hazard models to estimate hazard ratios (HRs) of having an incident fractures according to antihypertensive class and time since initiation.
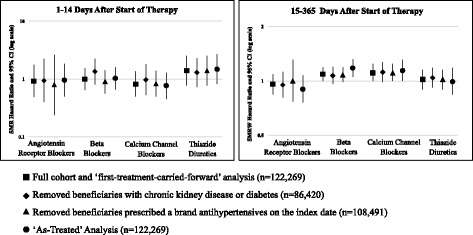
Results: During 2008-2011, 122,629 Medicare beneficiaries initiated antihypertensive monotherapy (mean age 75, 61% women, 86% White). Fracture rates varied according to days since initiation and antihypertensive class. Beneficiaries initiating with thiazides had the highest fracture rate in the first 14 days following initiation (438 per 10,000 person-years, 95% confidence interval (CI): 294-628; HR: 1.40, 0.78-2.52). However, beneficiaries initiating with calcium channel blockers had the highest fracture rate during the 15-365 days after initiation (435 per 10,000 person-years, 95% CI: 404-468; HR: 1.11, 1.00-1.24). Beneficiaries initiating with angiotensin-receptor blockers had the lowest fracture rates during the initial 14 days (333 per 10,000 person-years, 190-546, HR: 0.92, 0.49-1.75) and during 15-365 days after initiation (321 per 10,000 person-years, 287-358, HR: 0.96, 0.84-1.09).
Conclusion: The association between antihypertensives and fractures varied according to class and time since initiation. Results suggest that when deciding upon antihypertensive therapy, clinicians may want to consider possible fracture risks when choosing between antihypertensive drug classes.
Keywords: Antihypertensive initiation; Epidemiology; Fractures; Older adults.
Conflict of interest statement
Ethics approval and consent to participate
Medicare data were obtained under a data use agreement established with the Centers for Medicaid and Medicare Services (CMS) and the University of North Carolina at Chapel Hill (UNC-CH). The study protocol was approved by UNC’s Non-Biomedical Institutional Review Board (# 15-1704).
Consent for publication
Not applicable.
Competing interests
TS receives investigator-initiated research funding and support as Principal Investigator from the National Institute on Aging (NIA), and as Co-Investigator, National Institutes of Health (NIH). He also receives salary support as Director of the Comparative Effectiveness Research (CER) Strategic Initiative, NC TraCS Institute, UNC Clinical and Translational Science Award and as Director of the Center for Pharmacoepidemiology (current members: GlaxoSmithKline, UCB BioSciences, Merck) and research support from pharmaceutical companies (Amgen, AstraZeneca) to the Department of Epidemiology, University of North Carolina at Chapel Hill. Dr. Stürmer does not accept personal compensation of any kind from any pharmaceutical company. He owns stock in Novartis, Roche, BASF, AstraZeneca, and Novo Nordisk.
The authors declare that they have no competing interests.
Figures
References
-
- Annest JL, Fingerhut LA, Gallagher SS, Grossman DC, Hedegaard H, Johnson RL, Trent RB. Strategies to improve external cause-of-injury coding in state-based hospital discharge and emergency department data systems: recommendations of the CDC workgroup for improvement of external cause-of-injury coding. MMWR Recomm Rep. 2008;57(RR-1):1–15. - PubMed
-
- Aung K, Htay T. Thiazide diuretics and the risk of hip fracture. Cochrane Libr. 2011;(10). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
