

Eosinophilia and clinical outcome of chronic obstructive pulmonary disease: a meta-analysis
- PMID: 29044160
- PMCID: PMC5647332
- DOI: 10.1038/s41598-017-13745-x
Eosinophilia and clinical outcome of chronic obstructive pulmonary disease: a meta-analysis
Abstract
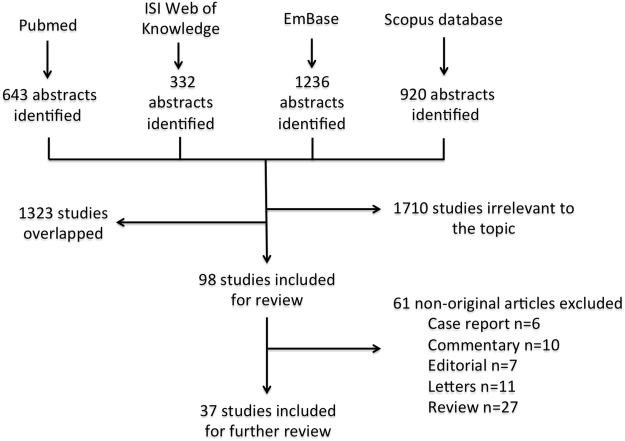
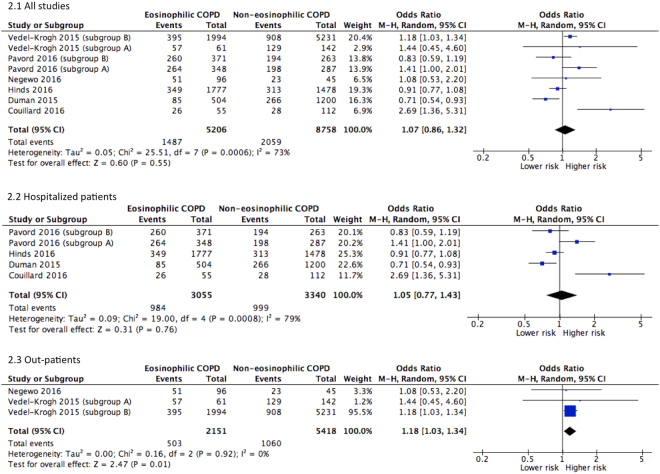
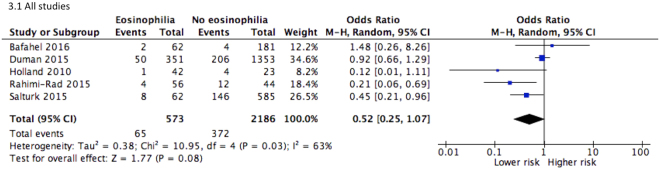
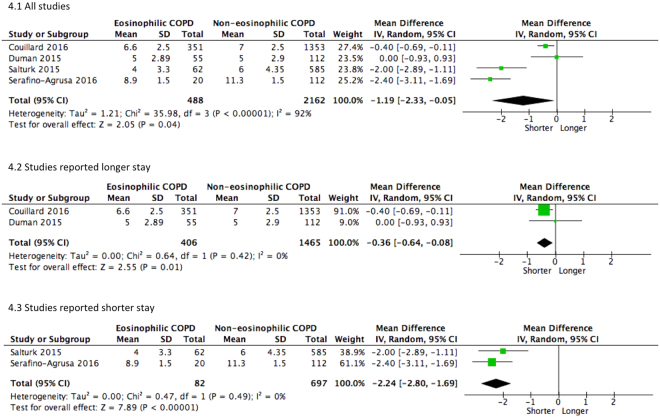
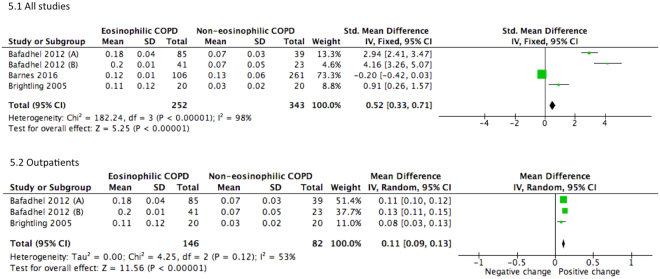
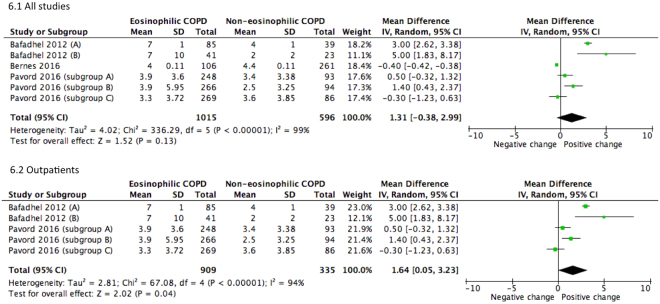
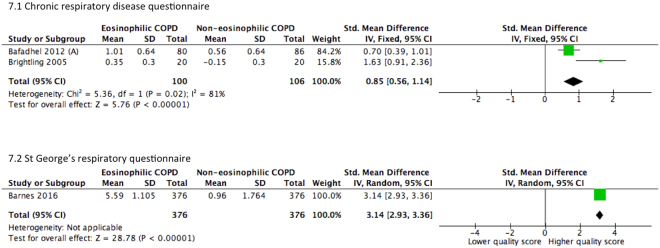
Numerous studies have investigated the association between eosinophilia and clinical outcome of patients with chronic obstructive pulmonary disease (COPD) but the evidence is conflicting. We conducted a pooled analysis of outcome measures comparing eosinophilic and non-eosinophilic COPD patients. We searched articles indexed in four databases using Medical Subject Heading or Title and Abstract words including COAD, COPD, eosinophil, eosinophilia, eosinopenia from inception to December 2016. Observational studies and randomized controlled trials with parallel groups comparing COPD patients with and without eosinophilia were included. Comparing to the non-eosinophilic group, those with eosinophilic COPD had a similar risk for exacerbation in 12 months [Odds ratio = 1.07, 95% confidence interval (CI) 0.86-1.32, P = 0.55] and in-hospital mortality [OR = 0.52, 95% CI 0.25-1.07]. Eosinophilia was associated with reduced length of hospital stay (P = 0.04). Subsequent to therapeutic interventions, eosinophilic outpatients performed better in pulmonary function tests [Mean Difference = 1.64, 95% CI 0.05-3.23, P < 0.001]. Inclusion of hospitalized patients nullified the effect. Improvement of quality of life was observed in eosinophilic subjects [Standardized Mean Difference = 1.83, 95% CI 0.02-3.64, P = 0.05], independent of hospitalization status. In conclusion, blood eosinophilia may be predictive of favorable response to steroidal and bronchodilator therapies in patients with stable COPD.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gorska K, et al. Eosinophilic airway inflammation in chronic obstructive pulmonary disease and asthma. J Physiol Pharmacol. 2008;59(Suppl 6):261–270. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
