

The advantages of intermediate-tier, inter-optometric referral of low risk pigmented lesions
- PMID: 29044669
- PMCID: PMC6446908
- DOI: 10.1111/opo.12413
The advantages of intermediate-tier, inter-optometric referral of low risk pigmented lesions
Abstract
Purpose: Pigmented ocular lesions are commonly encountered by eye-care professionals, and range from benign to sight or life-threatening. After identifying a lesion, the primary care professional must establish the likely diagnosis and decide either to reassure, to monitor or to refer. The increasing use of ocular imaging technologies has contributed to an increase in the detection rate of pigmented lesions and a higher number of referrals, which may challenge existing pathways of health-care delivery. Specialist services may be over-burdened by referring all patients with pigmented lesions for an opinion, while inter-optometric referrals are underutilised. The aim of this study was to describe the referral patterns of pigmented lesions to an optometry led intermediate-tier collaborative care clinic.
Methods: We performed a retrospective review of patient records using the list of patients examined at Centre for Eye Health (CFEH) for an initial or follow up pigmented lesion assessment between the 1/7/2013 and the 30/6/2016. Analysis was performed on: patient demographic characteristics, the referrer's tentative diagnosis, CFEH diagnosis and recommended management plan.
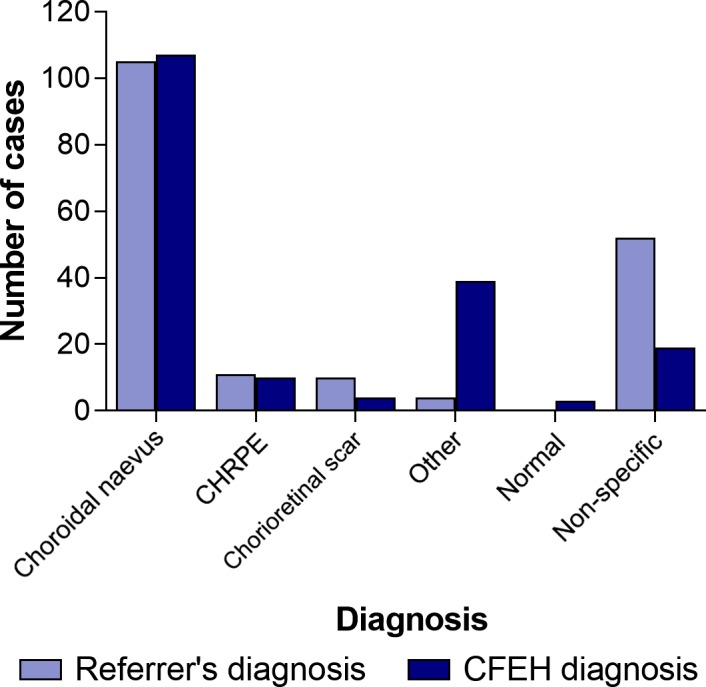
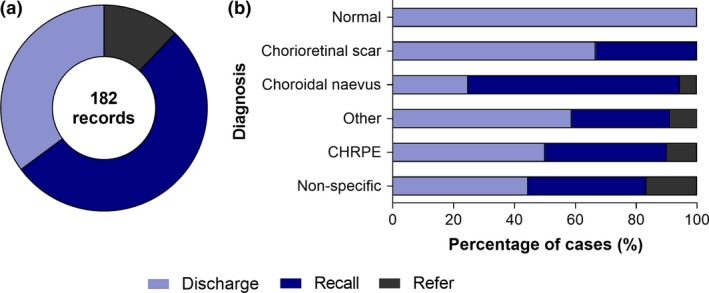
Results: Across 182 patient records, the primary lesion prompting referral was usually located in the posterior segment: choroidal naevus (105/182, 58%), congenital hypertrophy of the retinal pigment epithelium (CHRPE; 11/182, 6%), chorioretinal scarring (10/182, 5%) or not specified (52/182, 29%). Referrals described a specific request for ocular imaging in 25 instances (14%). The number of cases with a non-specific diagnosis was reduced after intermediate-tier care assessment (from 29% to 10%), while the number of diagnoses with less common conditions rose (from 2% to 21%). There was a 2% false positive referral rate to intermediate-tier care and a first visit discharge rate of 35%. A minority required on-referral to an ophthalmologist (22/182, 12%), either for unrelated incidental ocular findings, or suspicious choroidal naevi. Conditions most amenable to optometric follow up included: 1) chorioretinal scarring, 2) choroidal naevus, and 3) CHRPE.
Conclusions: Intermediate-tier optometric eye-care in pigmented lesions (following opportunistic primary care screening) has the potential to reduce the number of cases with non-specific diagnoses and to increase those with less common diagnoses. The majority of cases seen under this intermediate-tier model required only ongoing optometric surveillance.
Keywords: choroidal naevus; collaboration; pigmented lesions; shared-care.
© 2017 The Authors. Ophthalmic and Physiological Optics published by John Wiley & Sons Ltd on behalf of College of Optometrists.
Figures
Similar articles
-
The effectiveness of interventions for optometric referrals into the hospital eye service: A review.Ophthalmic Physiol Opt. 2023 Nov;43(6):1510-1523. doi: 10.1111/opo.13219. Epub 2023 Aug 25. Ophthalmic Physiol Opt. 2023. PMID: 37632154 Free PMC article. Review.
-
Collaborative care of non-urgent macular disease: a study of inter-optometric referrals.Ophthalmic Physiol Opt. 2016 Nov;36(6):632-642. doi: 10.1111/opo.12322. Ophthalmic Physiol Opt. 2016. PMID: 27790767 Free PMC article.
-
Clinical model assisting with the collaborative care of glaucoma patients and suspects.Clin Exp Ophthalmol. 2015 May-Jun;43(4):308-19. doi: 10.1111/ceo.12466. Epub 2014 Nov 25. Clin Exp Ophthalmol. 2015. PMID: 25362898
-
Clinical outcomes of the Centre for Eye Health: an intra-professional optometry-led collaborative eye care clinic in Australia.Clin Exp Optom. 2021 Sep;104(7):795-804. doi: 10.1080/08164622.2021.1878821. Epub 2021 Feb 25. Clin Exp Optom. 2021. PMID: 33689627
-
Can the MOLES acronym and scoring system improve the management of patients with melanocytic choroidal tumours?Eye (Lond). 2023 Apr;37(5):830-836. doi: 10.1038/s41433-022-02143-x. Epub 2022 Jun 28. Eye (Lond). 2023. PMID: 35764877 Free PMC article. Review.
Cited by
-
Survey of Australian primary eyecare management of choroidal nevus patients.Optom Vis Sci. 2025 Jul 1;102(7):452-457. doi: 10.1097/OPX.0000000000002256. Epub 2025 Apr 21. Optom Vis Sci. 2025. PMID: 40266266 Free PMC article.
-
Spatial Analysis Reveals Vascular Changes in Retinal and Choroidal Vessel Perfusion in Intermediate AMD With Reticular Pseudodrusen.Invest Ophthalmol Vis Sci. 2024 Feb 1;65(2):33. doi: 10.1167/iovs.65.2.33. Invest Ophthalmol Vis Sci. 2024. PMID: 38386332 Free PMC article.
-
[Progressive pigmented fundus lesion after 23 years-Treatment or observation?].Ophthalmologie. 2023 Aug;120(8):851-856. doi: 10.1007/s00347-022-01729-w. Epub 2022 Oct 14. Ophthalmologie. 2023. PMID: 36241750 German. No abstract available.
-
Multispectral pattern recognition measures change in drusen area in age-related macular degeneration with high congruency to expert graders.Sci Rep. 2022 May 6;12(1):7442. doi: 10.1038/s41598-022-11070-6. Sci Rep. 2022. PMID: 35524159 Free PMC article.
-
The effectiveness of interventions for optometric referrals into the hospital eye service: A review.Ophthalmic Physiol Opt. 2023 Nov;43(6):1510-1523. doi: 10.1111/opo.13219. Epub 2023 Aug 25. Ophthalmic Physiol Opt. 2023. PMID: 37632154 Free PMC article. Review.
References
-
- Damato EM & Damato BE. Detection and time to treatment of uveal melanoma in the United Kingdom: an evaluation of 2,384 patients. Ophthalmology 2012; 119: 1582–1589. - PubMed
-
- Law C, Krema H & Simpson ER. Referral patterns of intraocular tumour patients to a dedicated Canadian ocular oncology department. Can J Ophthalmol 2012; 47: 254–261. - PubMed
-
- Khan J & Damato BE. Accuracy of choroidal melanoma diagnosis by general ophthalmologists: a prospective study. Eye (Lond) 2007; 21: 595–597. - PubMed
-
- Shields CL, Furuta M, Berman EL et al Choroidal nevus transformation into melanoma: analysis of 2514 consecutive cases. Arch Ophthalmol 2009; 127: 981–987. - PubMed
-
- Silva PS, Cavallerano JD, Haddad NM et al Comparison of nondiabetic retinal findings identified with nonmydriatic fundus photography vs ultrawide field imaging in an ocular telehealth program. JAMA Ophthalmol 2016; 134: 330–334. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
