

Optimal prandial timing of bolus insulin in diabetes management: a review
- PMID: 29044708
- PMCID: PMC5836969
- DOI: 10.1111/dme.13525
Optimal prandial timing of bolus insulin in diabetes management: a review
Abstract
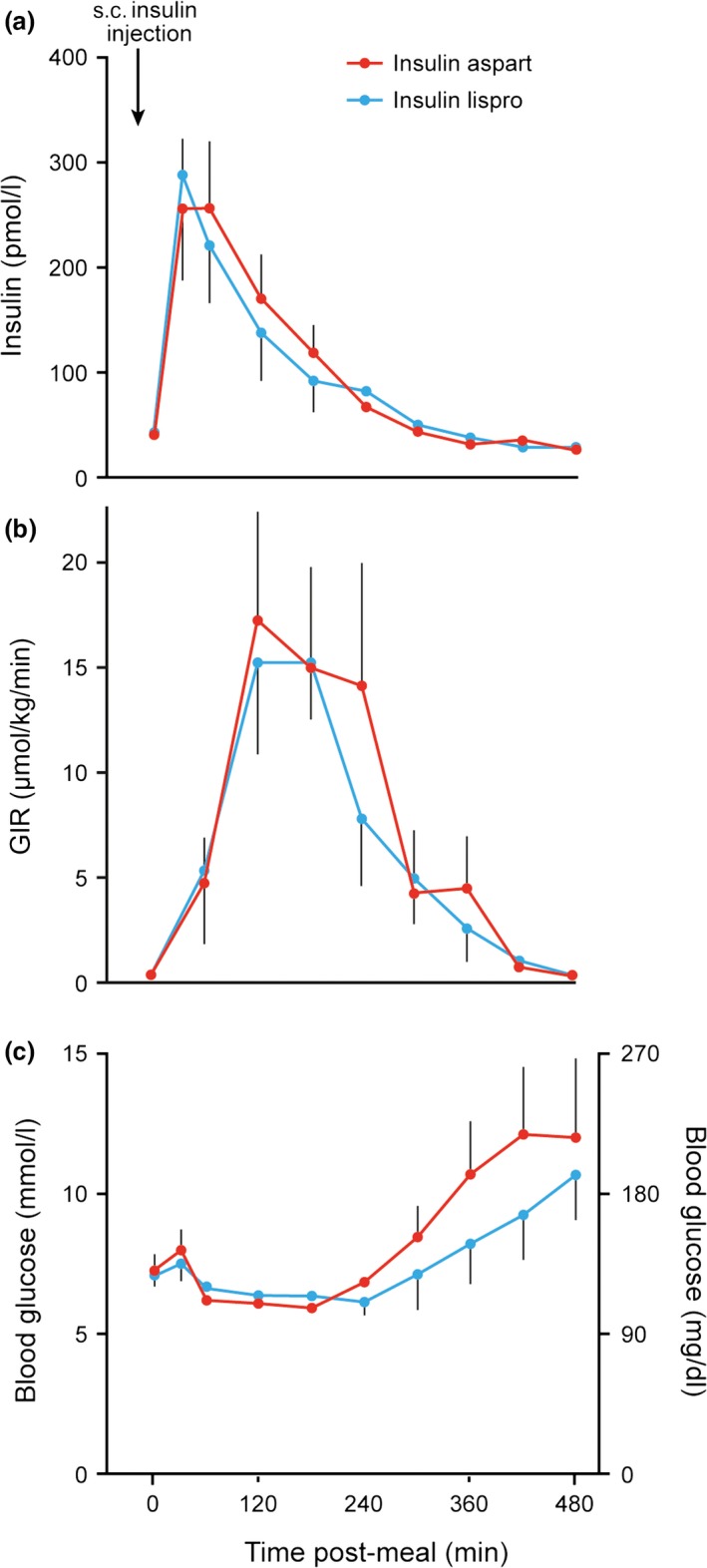
The inability to achieve optimal diabetes glucose control in people with diabetes is multifactorial, but one contributor may be inadequate control of postprandial glucose. In patients treated with multiple daily injections of insulin, both the dose and timing of meal-related rapid-acting insulin are key factors in this. There are conflicting opinions and evidence on the optimal time to administer mealtime insulin. We performed a comprehensive literature search to review the published data, focusing on the use of rapid-acting insulin analogues in patients with Type 1 diabetes. Pharmacokinetic and pharmacodynamic studies of rapid-acting insulin analogues, together with postprandial glucose excursion data, suggest that administering these 15-20 min before food would provide optimal postprandial glucose control. Data from clinical studies involving people with Type 1 diabetes receiving structured meals and rapid-acting insulin analogues support this, showing a reduction in post-meal glucose levels of ~30% and less hypoglycaemia when meal insulin was taken 15-20 min before a meal compared with immediately before the meal. Importantly, there was also a greater risk of postprandial hypoglycaemia when patients took rapid-acting analogues after eating compared with before eating.
© 2017 The Authors. Diabetic Medicine published by John Wiley & Sons Ltd on behalf of Diabetes UK.
Figures


References
-
- Diabetes Control and Complications Trial Research Group , Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O et al The effect of intensive treatment of diabetes on the development and progression of long‐term complications in insulin‐dependent diabetes mellitus. N Engl J Med 1993; 329: 977–986. - PubMed
-
- Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ et al Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group . Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005; 353: 2643–2653. - PMC - PubMed
-
- Health and Social Care Information Centre . National Diabetes Audit 2015‐2016. Report 1: Care Processes and Treatment Targets. 2013. Available at http://www.content.digital.nhs.uk/catalogue/PUB23241. Last accessed 18 June 2017.
-
- Ali MK, Bullard KM, Saaddine JB, Cowie CC, Imperatore G, Gregg EW. Achievement of goals in U.S. diabetes care, 1999–2010. N Engl J Med 2013; 368: 1613–1624. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
