

Inflammatory response and oxidative stress during liver resection
- PMID: 29045432
- PMCID: PMC5646773
- DOI: 10.1371/journal.pone.0185685
Inflammatory response and oxidative stress during liver resection
Abstract
Background: Postoperative complications are still a major concern after liver resection (LR). Systemic inflammation and deregulated reactive oxygen species during major abdominal surgery may impair outcome after hepatectomy.
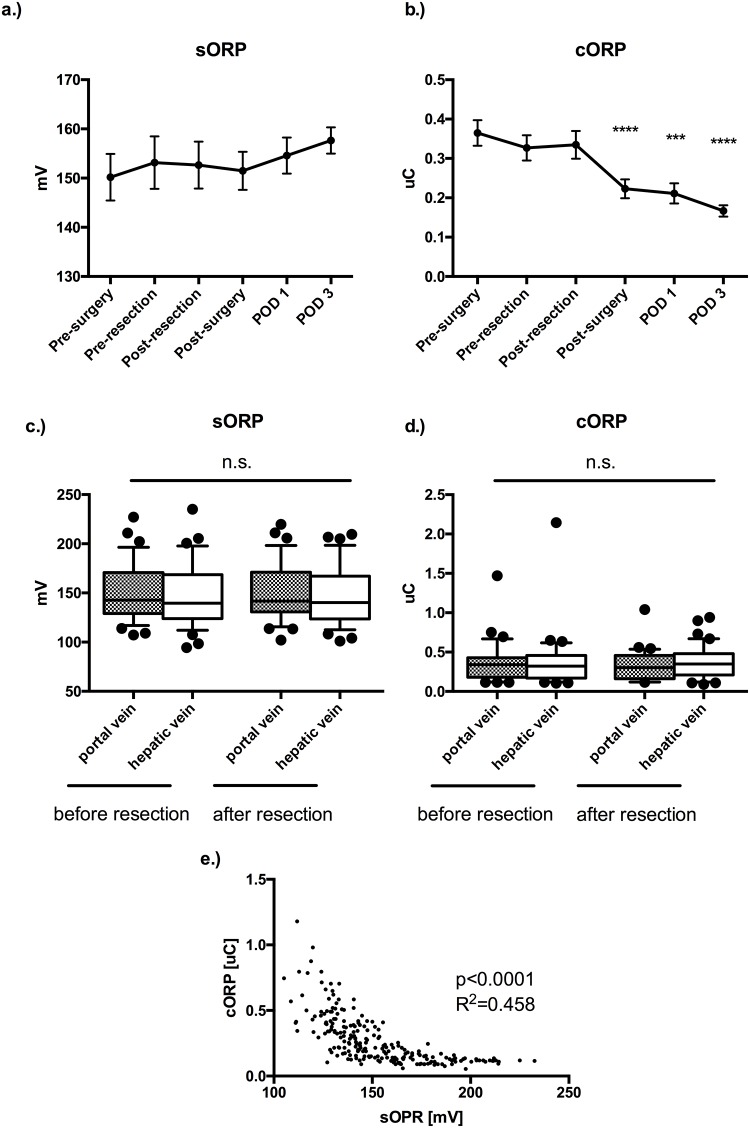
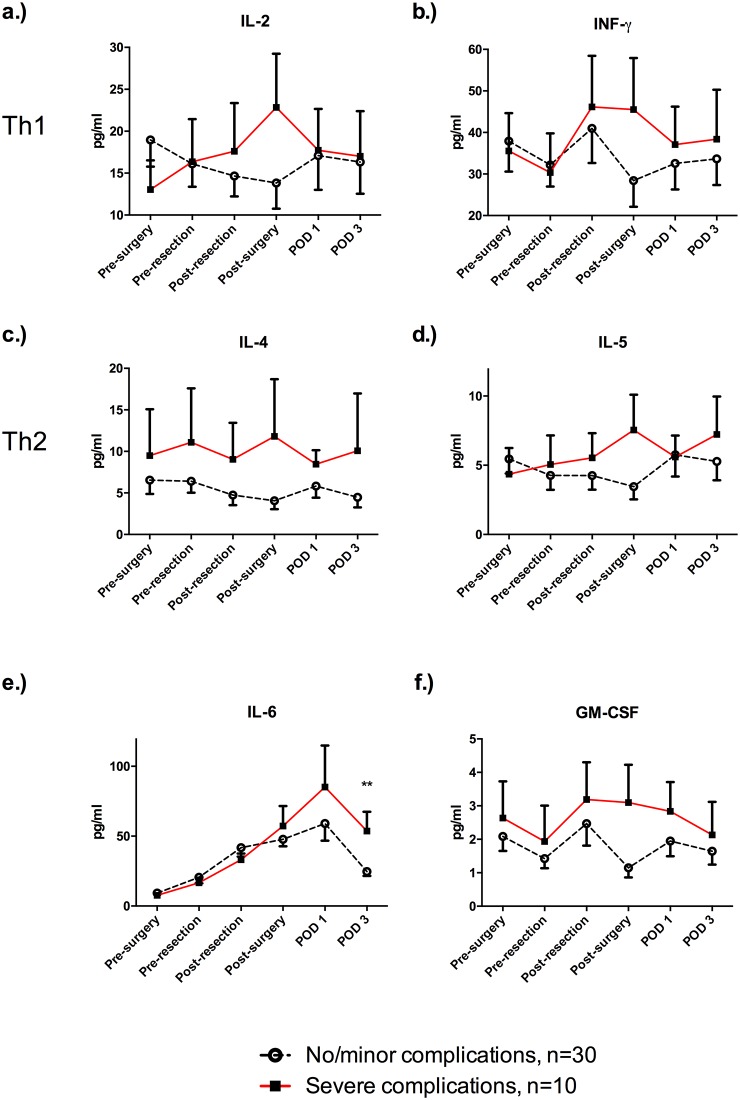
Methods: Patients undergoing LR were included in this study (n = 40). Oxidative stress (OS) was measured peri- and post-operatively as static oxidation-reduction potential markers (sORP) and antioxidant capacity ORP (cORP) by using the RedoxSYS Diagnostic system. Furthermore, Th1- and Th2-specific cytokines were assessed.
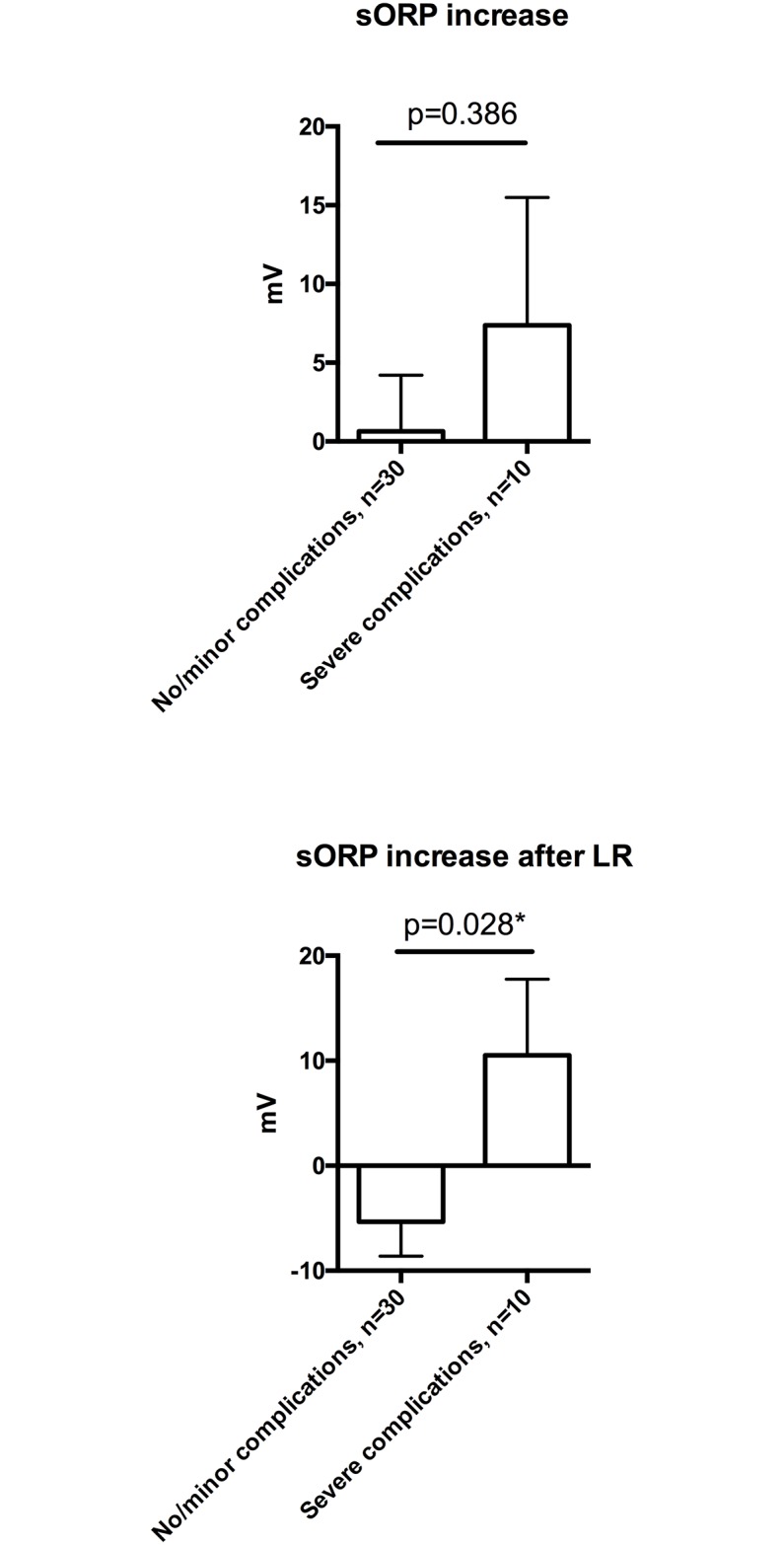
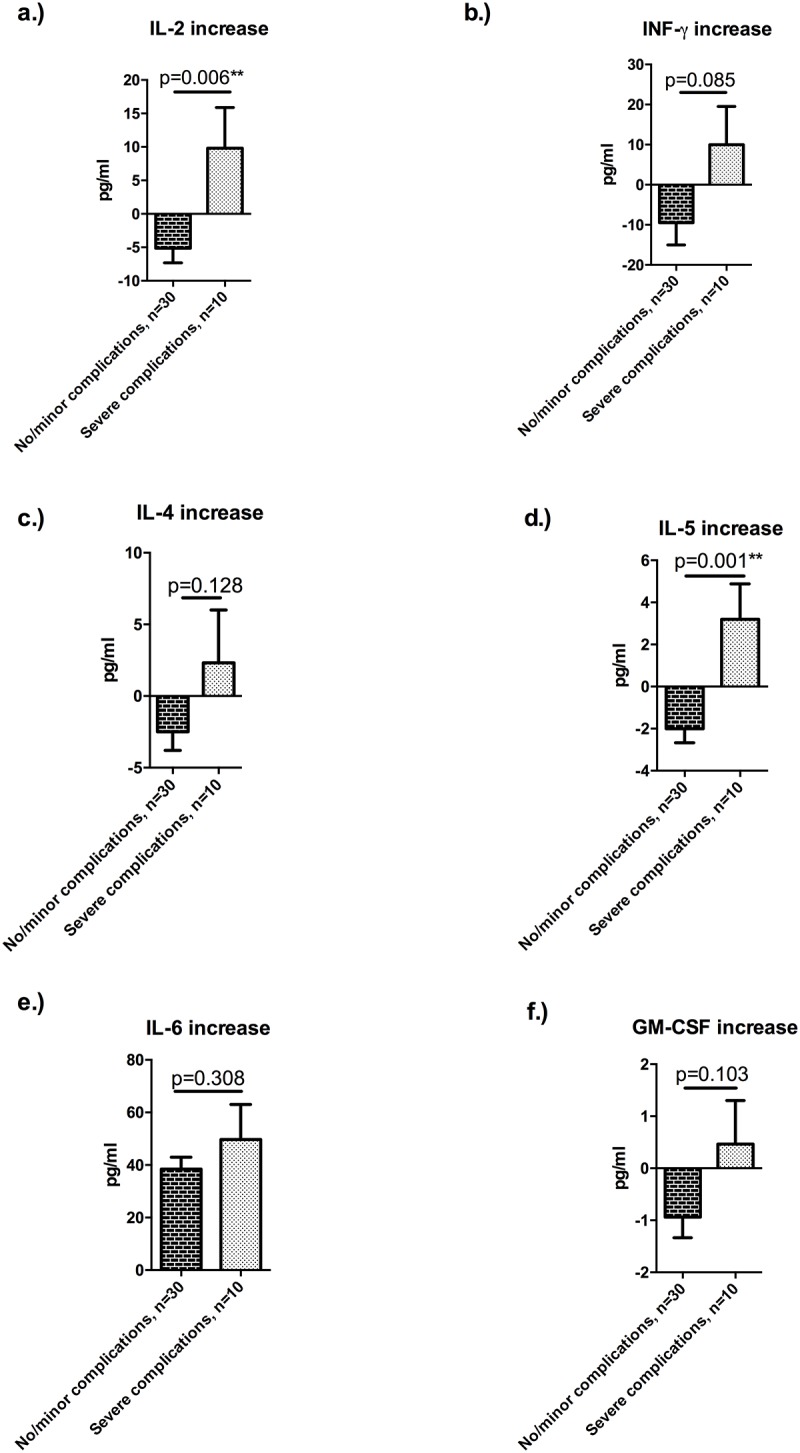
Results: Whereas there was no significant change in systemic sORP during LR and in the early postoperative course, there was a substantial decrease of cORP immediately post-surgery, and on postoperative days 1 and 3 (p<0.001). OS response was tightly regulated, as there was a significant correlation between sORP and cORP (p<0.0001; R2:0.457). An increase of OS (sORP) after LR of more than 3 mV was predictive for severe postoperative complications (53.8% vs. 12.5; p = 0.017). There was a significantly higher IL-2 (p = 0.006) and IL-5 (p = 0.001) increase during hepatectomy in patients who developed a severe morbidity.
Conclusion: Antioxidant capacity remained stable during LR but dropped during the post-surgical period, suggesting a consumption of antioxidants to maintain OS within healthy range. Severe postoperative complications were associated with a pronounced inflammatory response during surgery.
Conflict of interest statement
Figures
References
-
- Bleriot C, Dupuis T, Jouvion G, Eberl G, Disson O, Lecuit M. Liver-resident macrophage necroptosis orchestrates type 1 microbicidal inflammation and type-2-mediated tissue repair during bacterial infection. Immunity. 2015;42(1):145–58. doi: 10.1016/j.immuni.2014.12.020 - DOI - PubMed
-
- Gao B, Jeong WI, Tian Z. Liver: An organ with predominant innate immunity. Hepatology. 2008;47(2):729–36. doi: 10.1002/hep.22034 - DOI - PubMed
-
- Xu MJ, Feng D, Wu H, Wang H, Chan Y, Kolls J, et al. Liver is the major source of elevated serum lipocalin-2 levels after bacterial infection or partial hepatectomy: a critical role for IL-6/STAT3. Hepatology. 2015;61(2):692–702. doi: 10.1002/hep.27447 - DOI - PMC - PubMed
-
- Balmer ML, Slack E, de Gottardi A, Lawson MA, Hapfelmeier S, Miele L, et al. The liver may act as a firewall mediating mutualism between the host and its gut commensal microbiota. Science translational medicine. 2014;6(237):237ra66 doi: 10.1126/scitranslmed.3008618 - DOI - PubMed
-
- Clavien PA, Petrowsky H, DeOliveira ML, Graf R. Strategies for safer liver surgery and partial liver transplantation. The New England journal of medicine. 2007;356(15):1545–59. doi: 10.1056/NEJMra065156 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
