

Overall survival analysis of EXAM, a phase III trial of cabozantinib in patients with radiographically progressive medullary thyroid carcinoma
- PMID: 29045520
- PMCID: PMC5834040
- DOI: 10.1093/annonc/mdx479
Overall survival analysis of EXAM, a phase III trial of cabozantinib in patients with radiographically progressive medullary thyroid carcinoma
Abstract
Background: Primary analysis of the double-blind, phase III Efficacy of XL184 (Cabozantinib) in Advanced Medullary Thyroid Cancer (EXAM) trial demonstrated significant improvement in progression-free survival with cabozantinib versus placebo in patients with progressive medullary thyroid cancer (MTC). Final analysis of overall survival (OS), a key secondary endpoint, was carried out after long-term follow-up.
Patients and methods: EXAM compared cabozantinib with placebo in 330 patients with documented radiographic progression of metastatic MTC. Patients were randomized (2:1) to cabozantinib (140 mg/day) or placebo. Final OS and updated safety data are reported.
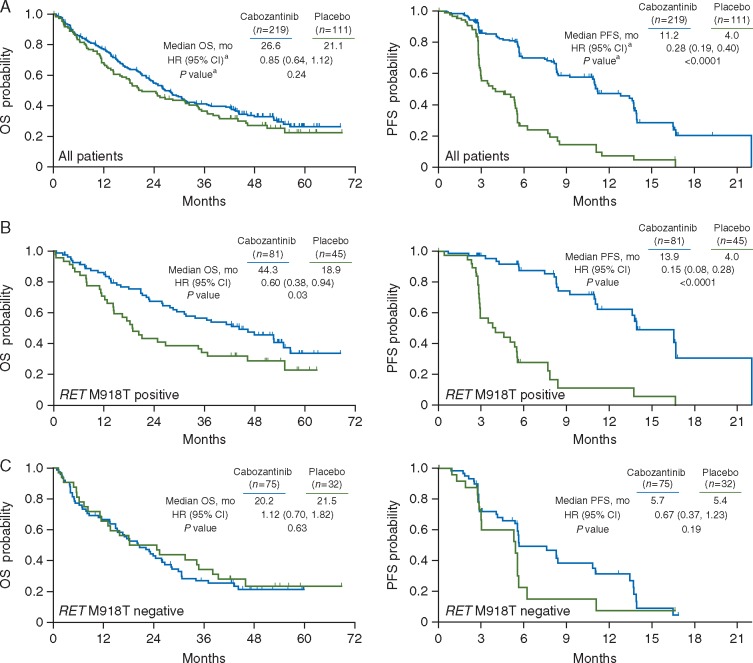
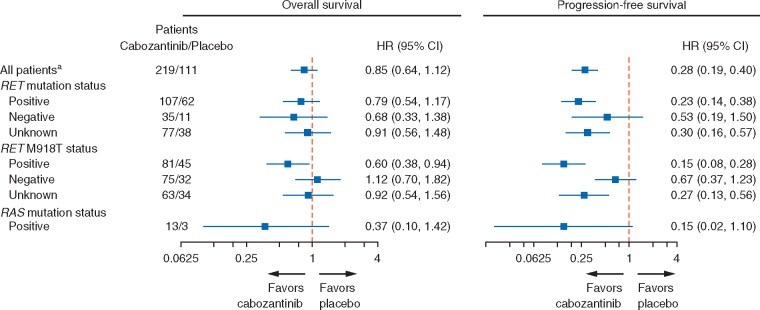
Results: Minimum follow-up was 42 months. Kaplan-Meier analysis showed a 5.5-month increase in median OS with cabozantinib versus placebo (26.6 versus 21.1 months) although the difference did not reach statistical significance [stratified hazard ratio (HR), 0.85; 95% confidence interval (CI), 0.64-1.12; P = 0.24]. In an exploratory assessment of OS, progression-free survival, and objective response rate, cabozantinib appeared to have a larger treatment effect in patients with RET M918T mutation-positive tumors compared with patients not harboring this mutation. For patients with RET M918T-positive disease, median OS was 44.3 months for cabozantinib versus 18.9 months for placebo [HR, 0.60; 95% CI, 0.38-0.94; P = 0.03 (not adjusted for multiple subgroup analyses)], with corresponding values of 20.2 versus 21.5 months (HR, 1.12; 95% CI, 0.70-1.82; P = 0.63) in the RET M918T-negative subgroup. Median treatment duration was 10.8 months with cabozantinib and 3.4 months with placebo. The safety profile for cabozantinib remained consistent with that of the primary analysis.
Conclusion: The secondary end point was not met in this final OS analysis from the trial of cabozantinib in patients with metastatic, radiographically progressive MTC. A statistically nonsignificant increase in OS was observed for cabozantinib compared with placebo. Exploratory analyses suggest that patients with RET M918T-positive tumors may experience a greater treatment benefit with cabozantinib.
Trial registration number: NCT00704730.
Keywords: RET M918T; cabozantinib; medullary thyroid cancer; overall survival; progression-free survival.
© The Author 2017. Published by Oxford University Press on behalf of the European Society for Medical Oncology. [br]All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Pusztaszeri MP, Bongiovanni M, Faquin WC.. Update on the cytologic and molecular features of medullary thyroid carcinoma. Adv Anat Pathol 2014; 21: 26–35. - PubMed
-
- Roman S, Lin R, Sosa JA.. Prognosis of medullary thyroid carcinoma: demographic, clinical, and pathologic predictors of survival in 1252 cases. Cancer 2006; 107: 2134–2142. - PubMed
-
- Links TP, Verbeek HH, Hofstra RM, Plukker JT.. Endocrine tumours: progressive metastatic medullary thyroid carcinoma: first- and second-line strategies. Eur J Endocrinol 2015; 172: R241–R251. - PubMed
-
- Kouvaraki MA, Shapiro SE, Perrier ND. et al. RET proto-oncogene: a review and update of genotype-phenotype correlations in hereditary medullary thyroid cancer and associated endocrine tumors. Thyroid 2005; 15: 531–544. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
