

Incidence, clinical management, and mortality risk following self harm among children and adolescents: cohort study in primary care
- PMID: 29046278
- PMCID: PMC5641980
- DOI: 10.1136/bmj.j4351
Incidence, clinical management, and mortality risk following self harm among children and adolescents: cohort study in primary care
Abstract
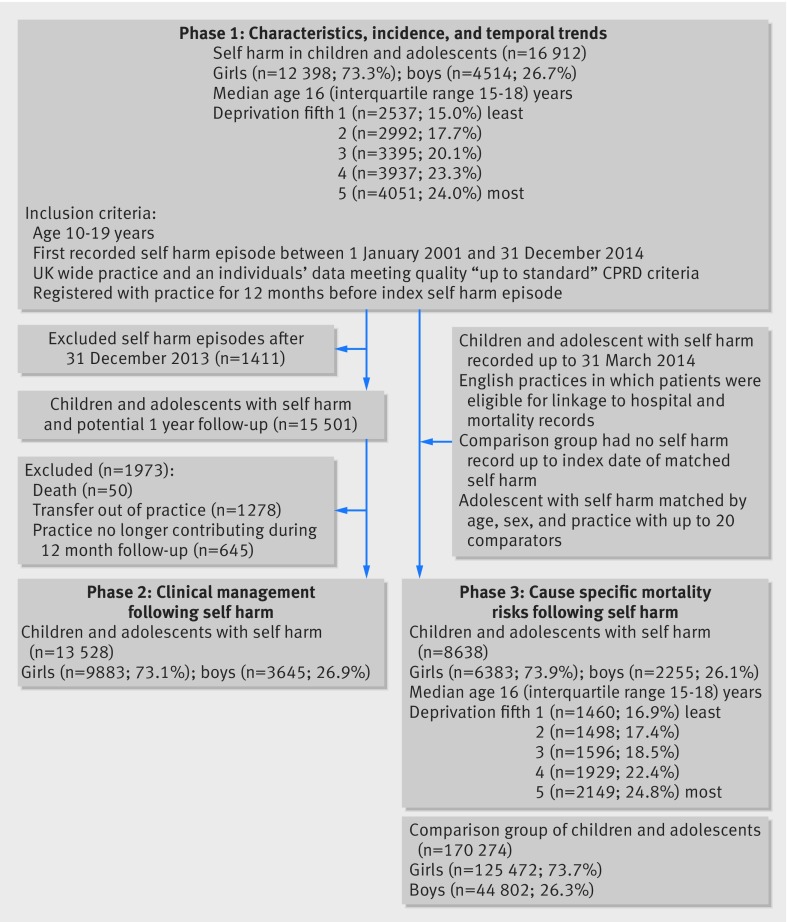
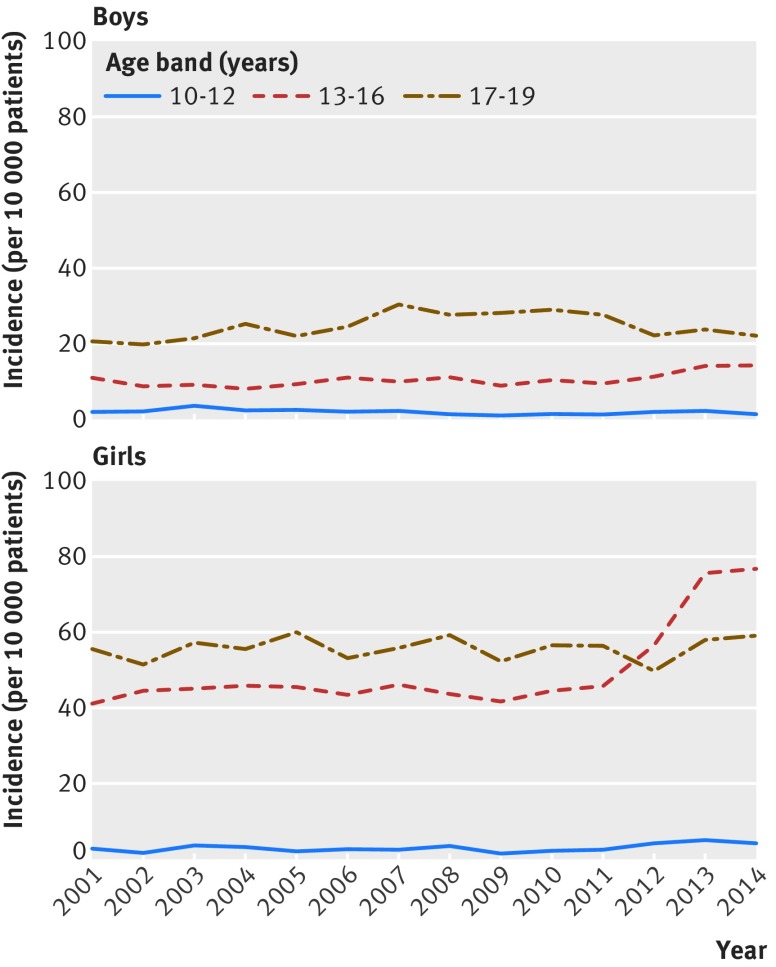
Objectives To examine temporal trends in sex and age specific incidence of self harm in children and adolescents, clinical management patterns, and risk of cause specific mortality following an index self harm episode at a young age.Design Population based cohort study.Setting UK Clinical Practice Research Datalink-electronic health records from 647 general practices, with practice level deprivation measured ecologically using the index of multiple deprivation. Patients from eligible English practices were linked to hospital episode statistics (HES) and Office for National Statistics (ONS) mortality records.Participants For the descriptive analytical phases we examined data pertaining to 16 912 patients aged 10-19 who harmed themselves during 2001-14. For analysis of cause specific mortality following self harm, 8638 patients eligible for HES and ONS linkage were matched by age, sex, and general practice with up to 20 unaffected children and adolescents (n=170 274).Main outcome measures In the first phase, temporal trends in sex and age specific annual incidence were examined. In the second phase, clinical management was assessed according to the likelihood of referral to mental health services and psychotropic drug prescribing. In the third phase, relative risks of all cause mortality, unnatural death (including suicide and accidental death), and fatal acute alcohol or drug poisoning were estimated as hazard ratios derived from stratified Cox proportional hazards models for the self harm cohort versus the matched unaffected comparison cohort.Results The annual incidence of self harm was observed to increase in girls (37.4 per 10 000) compared with boys (12.3 per 10 000), and a sharp 68% increase occurred among girls aged 13-16, from 45.9 per 10 000 in 2011 to 77.0 per 10 000 in 2014. Referrals within 12 months of the index self harm episode were 23% less likely for young patients registered at the most socially deprived practices, even though incidences were considerably higher in these localities. Children and adolescents who harmed themselves were approximately nine times more likely to die unnaturally during follow-up, with especially noticeable increases in risks of suicide (deprivation adjusted hazard ratio 17.5, 95% confidence interval 7.6 to 40.5) and fatal acute alcohol or drug poisoning (34.3, 10.2 to 115.7).Conclusions Gaining a better understanding of the mechanisms responsible for the recent apparent increase in the incidence of self harm among early-mid teenage girls, and coordinated initiatives to tackle health inequalities in the provision of services to distressed children and adolescents, represent urgent priorities for multiple public agencies.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf. NK chaired the NICE self harm guidelines, quality standard topic expert group; is current chair of NICE adult depression guidelines, treatment and management committee, topic expert NICE suicide prevention guidelines, and member of the Department of Health Suicide Prevention Strategy Advisory Group. Views expressed in the paper are those of the authors and not those of NICE or Department of Health. The authors have no other relationships or activities that could appear to have influenced the submitted work
Figures
References
-
- Moran P, Coffey C, Romaniuk H, et al. The natural history of self-harm from adolescence to young adulthood: a population-based cohort study. Lancet 2012;379:236-43. 10.1016/S0140-6736(11)61141-0 pmid:22100201. - DOI - PubMed
-
- Mars B, Heron J, Crane C, et al. Differences in risk factors for self-harm with and without suicidal intent: findings from the ALSPAC cohort. J Affect Disord 2014;168:407-14. 10.1016/j.jad.2014.07.009 pmid:25108277. - DOI - PMC - PubMed
-
- Patton GC, Coffey C, Romaniuk H, et al. The prognosis of common mental disorders in adolescents: a 14-year prospective cohort study. Lancet 2014;383:1404-11. 10.1016/S0140-6736(13)62116-9 pmid:24439298. - DOI - PubMed
-
- Hawton K, Harriss L. Deliberate self-harm in young people: characteristics and subsequent mortality in a 20-year cohort of patients presenting to hospital. J Clin Psychiatry 2007;68:1574-83. 10.4088/JCP.v68n1017 pmid:17960975. - DOI - PubMed
-
- Patton GC, Coffey C, Sawyer SM, et al. Global patterns of mortality in young people: a systematic analysis of population health data. Lancet 2009;374:881-92. 10.1016/S0140-6736(09)60741-8 pmid:19748397. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical