

Colorectal cancer incidence in path_MLH1 carriers subjected to different follow-up protocols: a Prospective Lynch Syndrome Database report
- PMID: 29046738
- PMCID: PMC5635542
- DOI: 10.1186/s13053-017-0078-5
Colorectal cancer incidence in path_MLH1 carriers subjected to different follow-up protocols: a Prospective Lynch Syndrome Database report
Abstract
Background: We have previously reported a high incidence of colorectal cancer (CRC) in carriers of pathogenic MLH1 variants (path_MLH1) despite follow-up with colonoscopy including polypectomy.
Methods: The cohort included Finnish carriers enrolled in 3-yearly colonoscopy (n = 505; 4625 observation years) and carriers from other countries enrolled in colonoscopy 2-yearly or more frequently (n = 439; 3299 observation years). We examined whether the longer interval between colonoscopies in Finland could explain the high incidence of CRC and whether disease expression correlated with differences in population CRC incidence.
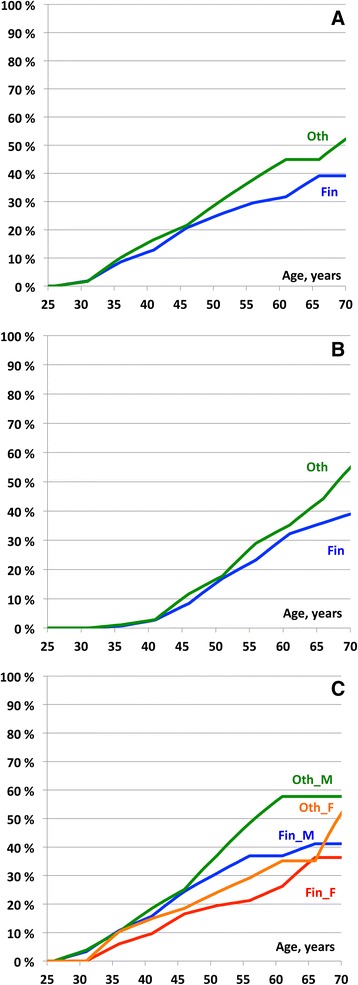
Results: Cumulative CRC incidences in carriers of path_MLH1 at 70-years of age were 41% for males and 36% for females in the Finnish series and 58% and 55% in the non-Finnish series, respectively (p > 0.05). Mean time from last colonoscopy to CRC was 32.7 months in the Finnish compared to 31.0 months in the non-Finnish (p > 0.05) and was therefore unaffected by the recommended colonoscopy interval. Differences in population incidence of CRC could not explain the lower point estimates for CRC in the Finnish series. Ten-year overall survival after CRC was similar for the Finnish and non-Finnish series (88% and 91%, respectively; p > 0.05).
Conclusions: The hypothesis that the high incidence of CRC in path_MLH1 carriers was caused by a higher incidence in the Finnish series was not valid. We discuss whether the results were influenced by methodological shortcomings in our study or whether the assumption that a shorter interval between colonoscopies leads to a lower CRC incidence may be wrong. This second possibility is intriguing, because it suggests the dogma that CRC in path_MLH1 carriers develops from polyps that can be detected at colonoscopy and removed to prevent CRC may be erroneous. In view of the excellent 10-year overall survival in the Finnish and non-Finnish series we remain strong advocates of current surveillance practices for those with LS pending studies that will inform new recommendations on the best surveillance interval.
Keywords: Colorectal cancer; Hereditary non-polyposis colorectal cancer; Lynch syndrome; Microsatellite instability.
Conflict of interest statement
Ethics approval and consent to participate
All reporting centers obtained informed consent for genetic testing and surveillance procedures. De-identified data was exported for the current study. No named registry needing approval was established for the current study.
Consent for publication
Not applicable.
Competing interests
Toni Seppälä: a co-owner (20%) of Healthfund Finland Oy (educational and health care services in Finland, not related to patients or scope of this manuscript). Travel costs to a scientific meeting by Medtronic Finland.
John Burn: a patent for high speed low cost tumor profiling pending to John Burn and QuantuMDx.
All others: None declared.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Møller P, Seppälä T, Bernstein I, Holinski-Feder E, Sala P, Evans DG, et al. Cancer incidence and survival in lynch syndrome patients receiving colonoscopic and gynaecological surveillance: first report from the prospective lynch syndrome database. Gut. 2017;66:464–472. doi: 10.1136/gutjnl-2015-309675. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
