

The Complement System and Preeclampsia
- PMID: 29046976
- PMCID: PMC5849056
- DOI: 10.1007/s11906-017-0784-4
The Complement System and Preeclampsia
Abstract
Purpose of review: Preeclampsia affects 3-4% of pregnancies with few treatment options to reduce maternal and fetal harm. Recent evidence that targeting the complement system may be an effective therapeutic strategy in prevention or treatment of preeclampsia will be reviewed.
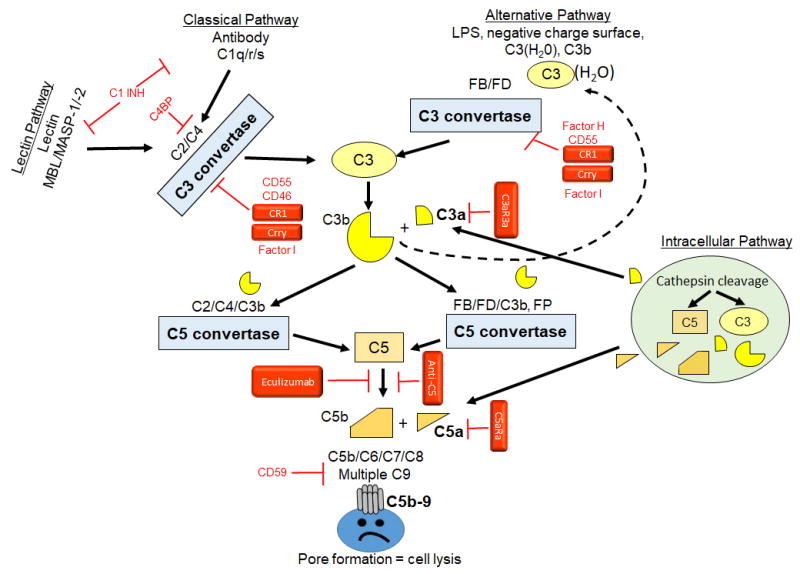
Recent findings: Studies in humans confirm the safety and efficacy of C5 blockade in complement-mediated disorders of pregnancy, including preeclampsia. Animal models mimic the placental abnormalities and/or the maternal symptoms which characterize preeclampsia. These models in mouse and rat have defined a role for complement and its regulators in placental dysfunction, hypertension, proteinuria, endothelial dysfunction, fetal growth restriction, and angiogenic imbalance, thus informing future human studies. Targeting excessive complement activation, particularly the terminal complement complex (C5b-9) and C5a may be an effective strategy to prolong pregnancy in women with preeclampsia. Continued research is needed to identify the initiator(s) of activation, the pathways involved, and the key component(s) in the pathophysiology to allow development of safe and effective therapeutics to target complement without compromising its role in homeostasis and host defense.
Keywords: Complement system; Innate immunity; Placenta; Placental ischemia; Preeclampsia; Pregnancy.
Figures
References
-
- Alsnes IV, Vatten LJ, Fraser A, Bjorngaard JH, Rich-Edwards J, Romundstad PR, et al. Hypertension in Pregnancy and Offspring Cardiovascular Risk in Young Adulthood: Prospective and Sibling Studies in the HUNT Study (Nord-Trondelag Health Study) in Norway. Hypertension. 2017;69(4):591–8. doi: 10.1161/HYPERTENSIONAHA.116.08414. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
