

Levosimendan for patients with severely reduced left ventricular systolic function and/or low cardiac output syndrome undergoing cardiac surgery: a systematic review and meta-analysis
- PMID: 29047417
- PMCID: PMC5648477
- DOI: 10.1186/s13054-017-1849-0
Levosimendan for patients with severely reduced left ventricular systolic function and/or low cardiac output syndrome undergoing cardiac surgery: a systematic review and meta-analysis
Abstract
Background: Previous studies have shown beneficial effects of levosimendan in high-risk patients undergoing cardiac surgery. Two large randomized controlled trials (RCTs), however, showed no advantages of levosimendan.
Methods: We performed a systematic review and meta-analysis (MEDLINE and Embase from inception until March 30, 2017), investigating whether levosimendan offers advantages compared with placebo in high-risk cardiac surgery patients, as defined by preoperative left ventricular ejection fraction (LVEF) ≤ 35% and/or low cardiac output syndrome (LCOS). The primary outcomes were mortality at longest follow-up and need for postoperative renal replacement therapy (RRT). Secondary postoperative outcomes investigated included myocardial injury, supraventricular arrhythmias, development of LCOS, acute kidney injury (AKI), duration of mechanical ventilation, intensive care unit and hospital lengths of stay, and incidence of hypotension during drug infusion.
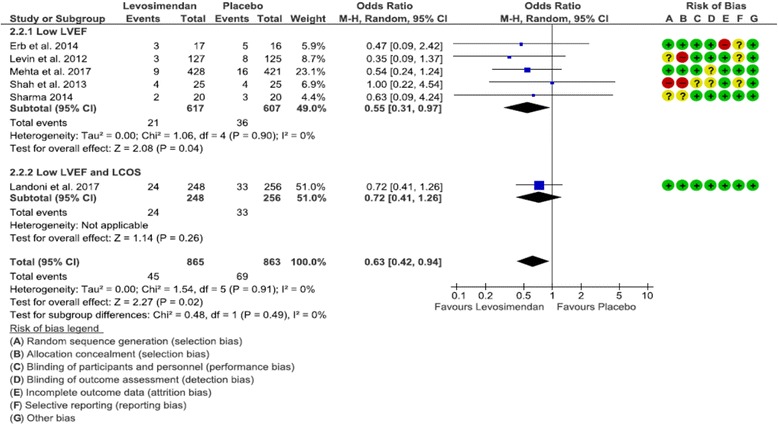
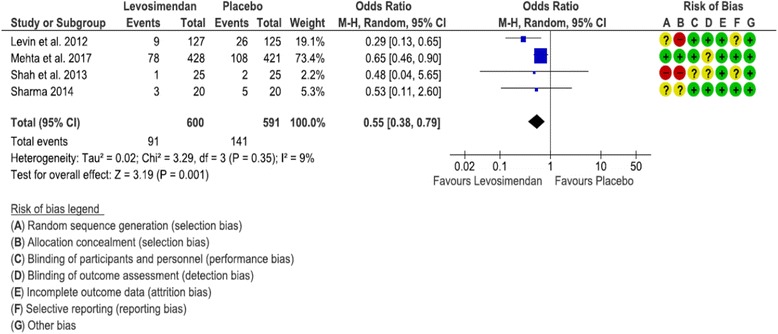
Results: Six RCTs were included in the meta-analysis, five of which investigated only patients with LVEF ≤ 35% and one of which included predominantly patients with LCOS. Mortality was similar overall (OR 0.64 [0.37, 1.11], p = 0.11) but lower in the subgroup with LVEF < 35% (OR 0.51 [0.32, 0.82], p = 0.005). Need for RRT was reduced by levosimendan both overall (OR 0.63 [0.42, 0.94], p = 0.02) and in patients with LVEF < 35% (OR 0.55 [0.31, 0.97], p = 0.04). Among secondary outcomes, we found lower postoperative LCOS in patients with LVEF < 35% receiving levosimendan (OR 0.49 [0.27, 0.89], p = 0.02), lower overall AKI (OR 0.62 [0.42, 0.92], p = 0.02), and a trend toward lower mechanical support, both overall (p = 0.07) and in patients with LVEF < 35% (p = 0.05).
Conclusions: Levosimendan reduces mortality in patients with preoperative severely reduced LVEF but does not affect overall mortality. Levosimendan reduces the need for RRT after high-risk cardiac surgery.
Keywords: Ejection fraction; Intensive care; Mortality; Renal replacement therapy.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Prophylactic levosimendan for the prevention of low cardiac output syndrome and mortality in paediatric patients undergoing surgery for congenital heart disease.Cochrane Database Syst Rev. 2017 Aug 2;8(8):CD011312. doi: 10.1002/14651858.CD011312.pub3. Cochrane Database Syst Rev. 2017. PMID: 28770972 Free PMC article.
-
Prophylactic levosimendan for the prevention of low cardiac output syndrome and mortality in paediatric patients undergoing surgery for congenital heart disease.Cochrane Database Syst Rev. 2017 Mar 6;3(3):CD011312. doi: 10.1002/14651858.CD011312.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2017 Aug 02;8:CD011312. doi: 10.1002/14651858.CD011312.pub3. PMID: 28262914 Free PMC article. Updated.
-
Inotropic agents and vasodilator strategies for the treatment of cardiogenic shock or low cardiac output syndrome.Cochrane Database Syst Rev. 2018 Jan 29;1(1):CD009669. doi: 10.1002/14651858.CD009669.pub3. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Nov 5;11:CD009669. doi: 10.1002/14651858.CD009669.pub4. PMID: 29376560 Free PMC article. Updated.
-
Levosimendan in Patients with Low Cardiac Output Syndrome After Cardiac Surgery: A Substudy of the Multicenter Randomized CHEETAH Trial.J Cardiothorac Vasc Anesth. 2025 Jan;39(1):151-161. doi: 10.1053/j.jvca.2024.10.003. Epub 2024 Oct 10. J Cardiothorac Vasc Anesth. 2025. PMID: 39482169 Clinical Trial.
-
Early levosimendan administration is associated with decreased mortality after cardiac surgery.J Crit Care. 2015 Aug;30(4):859.e1-6. doi: 10.1016/j.jcrc.2015.03.008. Epub 2015 Mar 13. J Crit Care. 2015. PMID: 25837801
Cited by
-
Impact of the perioperative inotropic support in grown-up congenital heart patients undergoing cardiac surgery: a propensity score adjusted analysis.Ann Intensive Care. 2020 Jul 9;10(1):91. doi: 10.1186/s13613-020-00709-0. Ann Intensive Care. 2020. PMID: 32648069 Free PMC article.
-
Association between levosimendan, postoperative AKI, and mortality in cardiac surgery: Insights from the LEVO-CTS trial.Am Heart J. 2021 Jan;231:18-24. doi: 10.1016/j.ahj.2020.10.066. Epub 2020 Oct 28. Am Heart J. 2021. PMID: 33127531 Free PMC article. Clinical Trial.
-
Levosimendan in Acute and Advanced Heart Failure: an Expert Perspective on Posology and Therapeutic Application.Cardiovasc Drugs Ther. 2018 Dec;32(6):617-624. doi: 10.1007/s10557-018-6838-2. Cardiovasc Drugs Ther. 2018. PMID: 30402660 Free PMC article. Review.
-
Prophylactic use of inotropic agents for the prevention of low cardiac output syndrome and mortality in adults undergoing cardiac surgery.Cochrane Database Syst Rev. 2024 Nov 27;11(11):CD013781. doi: 10.1002/14651858.CD013781.pub2. Cochrane Database Syst Rev. 2024. PMID: 39601298 Free PMC article.
-
A review of the management of patients with advanced heart failure in the intensive care unit.Ann Transl Med. 2020 Jul;8(13):828. doi: 10.21037/atm-20-1048. Ann Transl Med. 2020. PMID: 32793673 Free PMC article. Review.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, et al. Executive summary: heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):447–54. doi: 10.1161/CIR.0000000000000366. - DOI - PubMed
-
- Bridgewater B, Grayson AD, Brooks N, Grotte G, Fabri BM, Au J, Hooper T, Jones M, Keogh B. Has the publication of cardiac surgery outcome data been associated with changes in practice in northwest England: an analysis of 25,730 patients undergoing CABG surgery under 30 surgeons over eight years. Heart. 2007;93(6):744–8. doi: 10.1136/hrt.2006.106393. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
