

Excellent Treatment Outcomes in Children Treated for Tuberculosis Under Routine Operational Conditions in Cape Town, South Africa
- PMID: 29048512
- PMCID: PMC5850643
- DOI: 10.1093/cid/cix602
Excellent Treatment Outcomes in Children Treated for Tuberculosis Under Routine Operational Conditions in Cape Town, South Africa
Abstract
Background: Tuberculosis (TB) remains a leading cause of death in children globally. It is recognized that human immunodeficiency virus (HIV) infection increases the risk of developing TB, but our understanding of the impact of HIV on risk of mortality for children treated for TB is limited. We aimed to identify predictors of mortality in children treated for drug-susceptible TB.
Methods: A retrospective analysis of all children (<15 years of age) routinely treated between 2005 and 2012 for drug-susceptible TB in Cape Town was conducted using the programmatic electronic TB treatment database. Survival analysis using Cox regression was used to estimate hazard ratios for death. Logistic regression was used to estimate the odds of unfavorable outcomes.
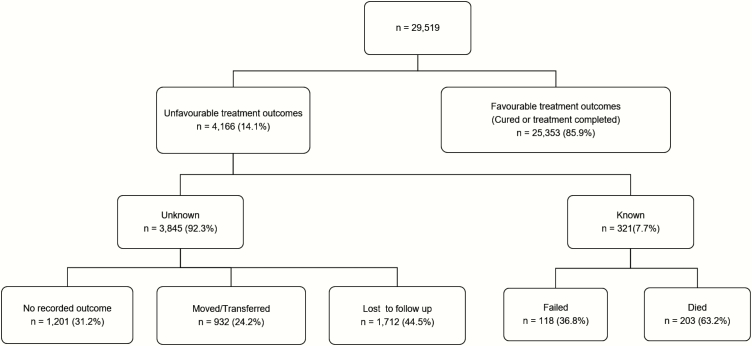
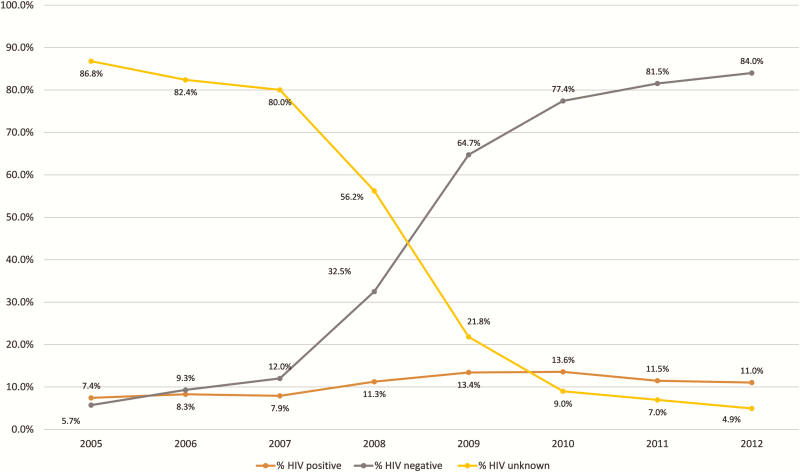
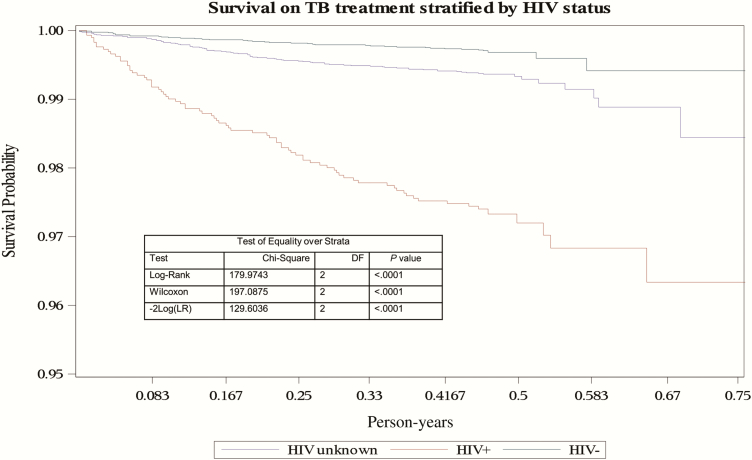
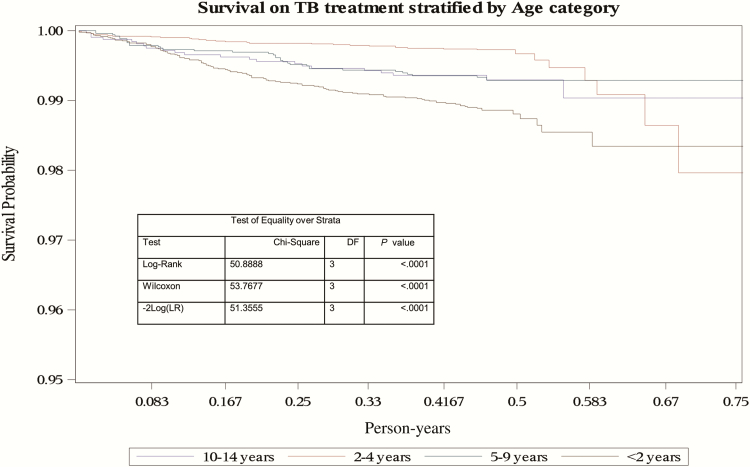
Results: Of 29519 children treated for and notified with TB over the study period, <1% died during TB treatment and 89.5% were cured or completed treatment. The proportion of children with known HIV status increased from 13% in 2005 to 95% in 2012. Children aged <2 years had an increased hazard of death (adjusted hazard ratio [aHR], 3.13; 95% confidence interval [CI], 1.78-5.52) and greater odds of unfavorable outcome (adjusted odds ratio [aOR], 1.44; 95% CI, 1.24-1.66) compared with children aged 10-14 years. HIV-infected children had increased mortality compared to HIV-negative children (aHR, 6.85; 95% CI, 4.60-10.19) and increased odds of unfavorable outcome (aOR, 2.01; 95% CI, 1.81-2.23). Later year of TB treatment was a protective predictor for both mortality and unfavorable outcome.
Conclusions: We demonstrate a dramatic improvement in HIV testing in children with TB over time and excellent overall treatment outcomes. HIV infection and young age were associated with increased risk of death and unfavorable outcome.
Keywords: childhood; mortality; outcomes; tuberculosis.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Nationwide analysis of treatment outcomes in children and adolescents routinely treated for tuberculosis in the Netherlands.Eur Respir J. 2019 Dec 12;54(6):1901402. doi: 10.1183/13993003.01402-2019. Print 2019 Dec. Eur Respir J. 2019. PMID: 31515410
-
Pediatric tuberculosis outcomes and factors associated with unfavorable treatment outcomes in Botswana, 2008-2019: a retrospective analysis.BMC Public Health. 2022 Nov 4;22(1):2020. doi: 10.1186/s12889-022-14477-y. BMC Public Health. 2022. PMID: 36333805 Free PMC article.
-
Survival and predictors of mortality among children co-infected with tuberculosis and human immunodeficiency virus at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. A retrospective follow-up study.PLoS One. 2018 May 22;13(5):e0197145. doi: 10.1371/journal.pone.0197145. eCollection 2018. PLoS One. 2018. PMID: 29787596 Free PMC article.
-
Tuberculosis Treatment Outcomes Among Children in Rural Southern Mozambique: A 12-year Retrospective Study.Pediatr Infect Dis J. 2019 Oct;38(10):999-1004. doi: 10.1097/INF.0000000000002435. Pediatr Infect Dis J. 2019. PMID: 31568138 Free PMC article.
-
Effect of HIV status and antiretroviral treatment on treatment outcomes of tuberculosis patients in a rural primary healthcare clinic in South Africa.PLoS One. 2022 Oct 12;17(10):e0274549. doi: 10.1371/journal.pone.0274549. eCollection 2022. PLoS One. 2022. PMID: 36223365 Free PMC article. Review.
Cited by
-
Factors Determining Treatment Success in Children with Drug-Sensitive Tuberculosis in Ethiopia: A Three-Year Retrospective Analysis.Am J Trop Med Hyg. 2020 Nov;103(5):1813-1817. doi: 10.4269/ajtmh.19-0816. Am J Trop Med Hyg. 2020. PMID: 32959757 Free PMC article.
-
Clinical Outcomes in Children With Human Immunodeficiency Virus Treated for Nonsevere Tuberculosis in the SHINE Trial.Clin Infect Dis. 2024 Jul 19;79(1):70-77. doi: 10.1093/cid/ciae193. Clin Infect Dis. 2024. PMID: 38592950 Free PMC article. Clinical Trial.
-
Inclusion of key populations in clinical trials of new antituberculosis treatments: Current barriers and recommendations for pregnant and lactating women, children, and HIV-infected persons.PLoS Med. 2019 Aug 15;16(8):e1002882. doi: 10.1371/journal.pmed.1002882. eCollection 2019 Aug. PLoS Med. 2019. PMID: 31415563 Free PMC article.
-
Mortality in South African Children and Adolescents Routinely Treated for Tuberculosis.Pediatrics. 2021 Apr;147(4):e2020032490. doi: 10.1542/peds.2020-032490. Epub 2021 Mar 10. Pediatrics. 2021. PMID: 33692161 Free PMC article.
-
Effect of First-Line Antituberculosis Therapy on Nevirapine Pharmacokinetics in Children Younger than Three Years Old.Antimicrob Agents Chemother. 2019 Sep 23;63(10):e00839-19. doi: 10.1128/AAC.00839-19. Print 2019 Oct. Antimicrob Agents Chemother. 2019. PMID: 31332062 Free PMC article.
References
-
- World Health Organization. Global tuberculosis report (2016). Geneva, Switzerland: WHO, 2016.
-
- Dodd PJ, Sismanidis C, Seddon JA. Global burden of drug-resistant tuberculosis in children: a mathematical modelling study. Lancet Infect Dis 2016; 16:1193–201. - PubMed
-
- Marais BJ, Gie RP, Schaaf HS et al. . The natural history of childhood intra-thoracic tuberculosis: a critical review of literature from the pre-chemotherapy era. Int J Tuberc Lung Dis 2004; 8:392–402. - PubMed
-
- Chiang SS, Khan FA, Milstein MB et al. . Treatment outcomes of childhood tuberculous meningitis: a systematic review and meta-analysis. Lancet Infect Dis 2014; 14:947–57. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
