

Impact of Enhanced Recovery After Surgery and Opioid-Free Anesthesia on Opioid Prescriptions at Discharge From the Hospital: A Historical-Prospective Study
- PMID: 29049123
- PMCID: PMC7402216
- DOI: 10.1213/ANE.0000000000002510
Impact of Enhanced Recovery After Surgery and Opioid-Free Anesthesia on Opioid Prescriptions at Discharge From the Hospital: A Historical-Prospective Study
Abstract
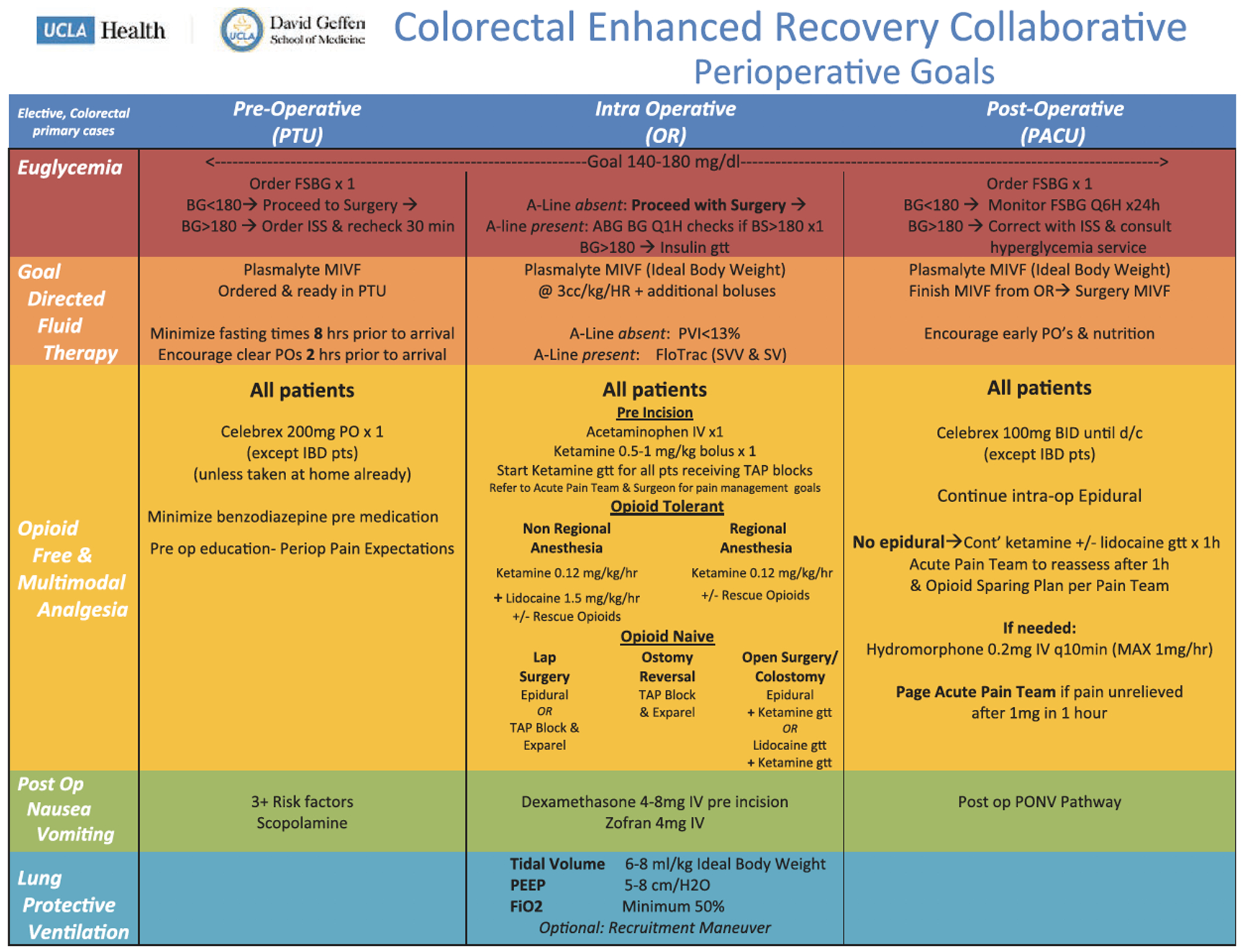
Background: The United States is in the midst of an opioid epidemic, and opioid use disorder often begins with a prescription for acute pain. The perioperative period represents an important opportunity to prevent chronic opioid use, and recently there has been a paradigm shift toward implementation of enhanced recovery after surgery (ERAS) protocols that promote opioid-free and multimodal analgesia. The objective of this study was to assess the impact of an ERAS intervention for colorectal surgery on discharge opioid prescribing practices.
Methods: We conducted a historical-prospective quality improvement study of an ERAS protocol implemented for patients undergoing colorectal surgery with a focus on the opioid-free and multimodal analgesia components of the pathway. We compared patients undergoing colorectal surgery 1 year before implementation (June 15, 2015, to June 14, 2016) and 1 year after implementation (June 15, 2016, to June 14, 2017).
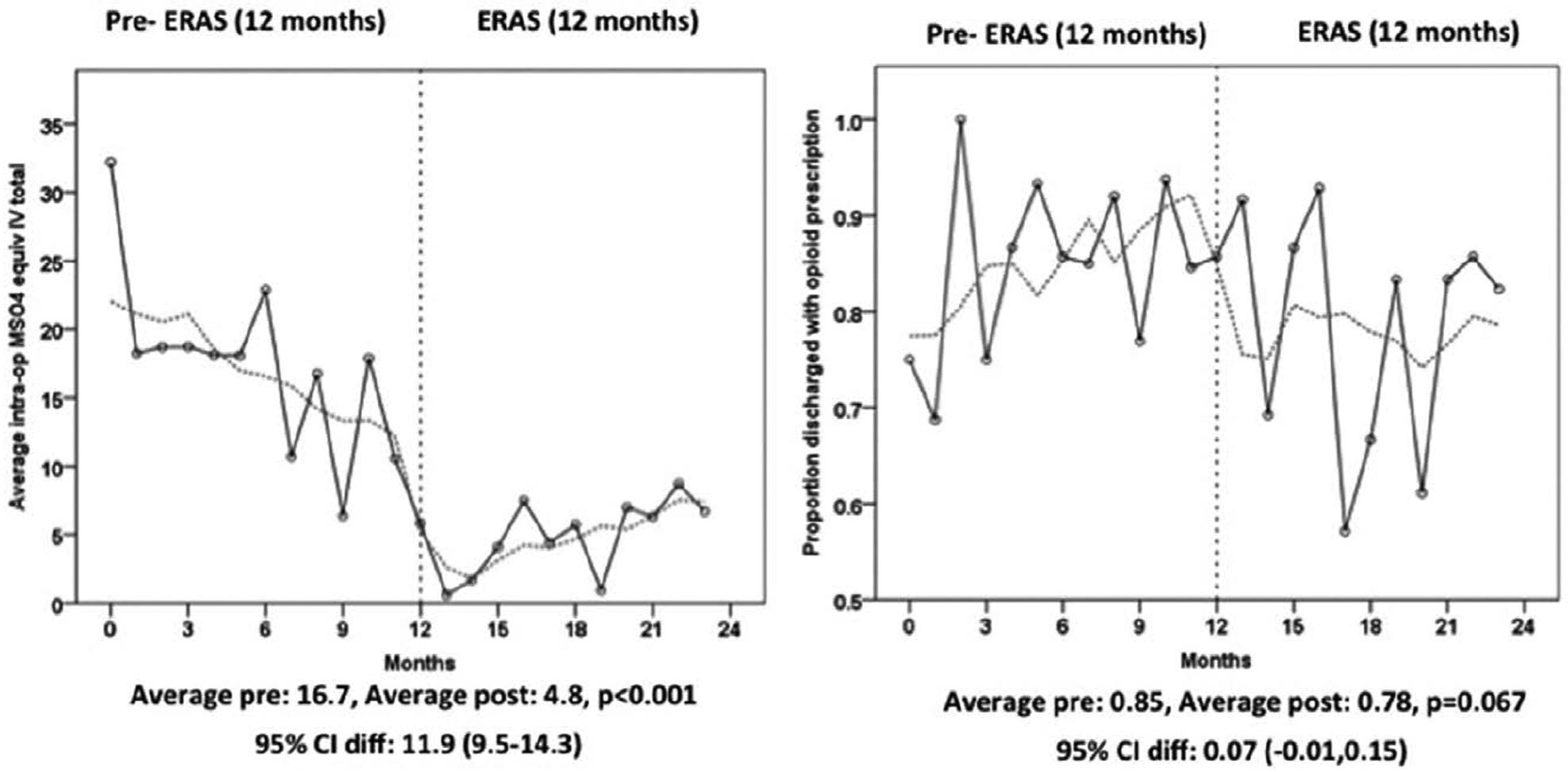
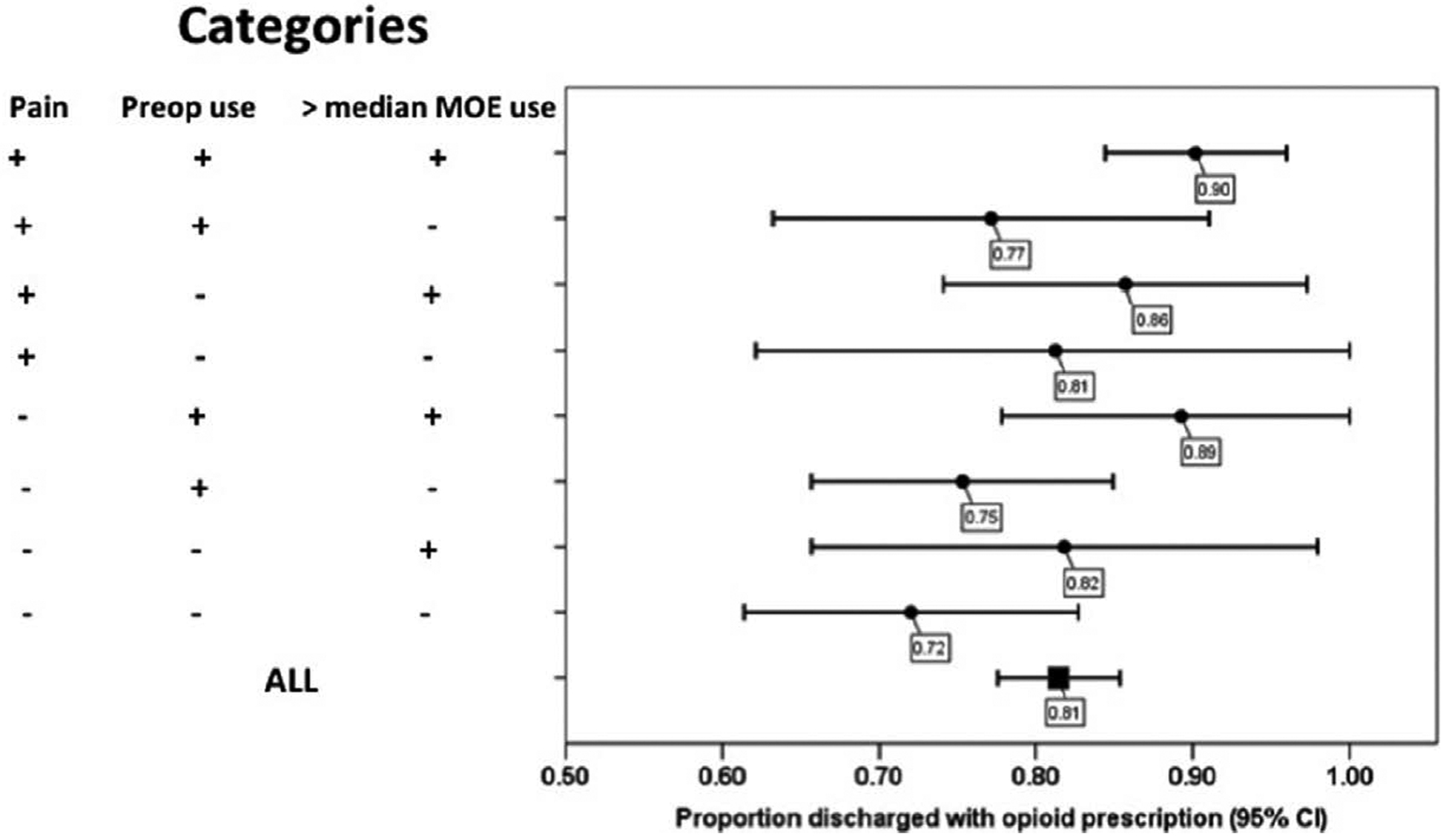
Results: Before the ERAS intervention, opioids at discharge were not significantly increasing (1% per month; 95% confidence interval [CI], -1% to 3%; P = .199). Immediately after the ERAS intervention, opioid prescriptions were not significantly lower (13%; 95% CI, -30% to 3%; P = .110). After the intervention, the rate of opioid prescriptions at discharge did not decrease significantly 1% (95% CI, -3% to 1%) compared to the pre-period rate (P = .399). Subgroup analysis showed that in patients with a combination of low discharge pain scores, no preoperative opioid use, and low morphine milligram equivalents consumption before discharge, the rate of discharge opioid prescription was 72% (95% CI, 61%-83%).
Conclusions: This study is the first to report discharge opioid prescribing practices in an ERAS setting. Although an ERAS intervention for colorectal surgery led to an increase in opioid-free anesthesia and multimodal analgesia, we did not observe an impact on discharge opioid prescribing practices. The majority of patients were discharged with an opioid prescription, including those with a combination of low discharge pain scores, no preoperative opioid use, and low morphine milligram equivalents consumption before discharge. This observation in the setting of an ERAS pathway that promotes multimodal analgesia suggests that our findings are very likely to also be observed in non-ERAS settings and offers an opportunity to modify opioid prescribing practices on discharge after surgery. For opioid-free anesthesia and multimodal analgesia to influence the opioid epidemic, the dose and quantity of the opioids prescribed should be modified based on the information gathered by in-hospital pain scores and opioid use as well as pain history before admission.
Conflict of interest statement
DISCLOSURES
Name: Delara Brandal, MD.
Contribution: This author helped edit the manuscript and implement the study.
Conflicts of Interest: None.
Name: Michelle S. Keller, MPH.
Contribution: This author helped edit the manuscript.
Conflicts of Interest: None.
Name: Carol Lee, RN-BC.
Contribution: This author helped edit the manuscript, create the ERAS pathway, and implement the study.
Conflicts of Interest: None.
Name: Tristan Grogan, MS.
Contribution: This author helped edit the manuscript and analyze the statistical data.
Conflicts of Interest: None.
Name: Yohei Fujimoto, MD, PhD.
Contribution: This author helped edit the manuscript, implement the study, and analyze the data.
Conflicts of Interest: None.
Name: Yann Gricourt, MD.
Contribution: This author helped edit the manuscript, implement the study, and analyze the data.
Conflicts of Interest: None.
Name: Takashige Yamada, MD, PhD.
Contribution: This author helped edit the manuscript, implement the study, and analyze the data.
Conflicts of Interest: None.
Name: Siamak Rahman, MD.
Contribution: This author helped edit the manuscript, create the ERAS pathway, and implement the study.
Conflicts of Interest: None.
Name: Ira Hofer, MD.
Contribution: This author helped edit the manuscript, create the ERAS pathway, implement the study, and collect the data.
Conflicts of Interest: None.
Name: Kevork Kazanjian, MD.
Contribution: This author helped edit the manuscript.
Conflicts of Interest: None.
Name: Jonathan Sack, MD.
Contribution: This author helped edit the manuscript.
Conflicts of Interest: None.
Name: Aman Mahajan, MD, PhD.
Contribution: This author helped edit the manuscript and advise on the project.
Conflicts of Interest: None.
Name: Anne Lin, MD.
Contribution: This author helped edit the manuscript, lead the project, and create the ERAS pathway.
Conflicts of Interest: None.
Name: Maxime Cannesson, MD, PhD.
Contribution: This author helped edit the manuscript, lead the project, and create the ERAS pathway.
Conflicts of Interest: Maxime Cannesson is an editor for the Technology, Computing, and Simulation section of Anesthesia & Analgesia.
Figures
References
-
- Bedard NA, Pugely AJ, Westermann RW, Duchman KR, Glass NA, Callaghan JJ. Opioid use after total knee arthroplasty: trends and risk factors for prolonged use. J Arthroplasty. 2017;32:2390–2394. - PubMed
-
- Kelly MA. Addressing the opioid epidemic with multimodal pain management. Am J Orthop (Belle Mead NJ). 2016;45:S6–S8. - PubMed
-
- Hedden S Behavioral Health Trends in the United States: Results From the 2014 National Survey on Drug Use and Health (HHS Publication No. SMA 15–4927, NSDUH Series H-50). Washington, DC: Substance Abuse and Mental Health Services Administration, Department of Health and Human Services; 2015.
-
- Johnson SP, Chung KC, Zhong L, et al. Risk of prolonged opioid use among opioid-naïve patients following common hand surgery procedures. J Hand Surg Am. 2016;41:947–957.e3. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
