

Comparison of Internal Medicine and General Surgery Residents' Assessments of Risk of Postsurgical Complications in Surgically Complex Patients
- PMID: 29049425
- PMCID: PMC5885933
- DOI: 10.1001/jamasurg.2017.3936
Comparison of Internal Medicine and General Surgery Residents' Assessments of Risk of Postsurgical Complications in Surgically Complex Patients
Abstract
Importance: Anticipating postsurgical complications is a vital physician skill, particularly when counseling surgically complex patients on their risks of intervention. Although internists and surgeons both counsel patients on surgical risks, it is uncertain who is better equipped to accurately anticipate surgical complications.
Objective: To examine how internal medicine and general surgery trainees compare in their assessment of risk of surgically complex patients.
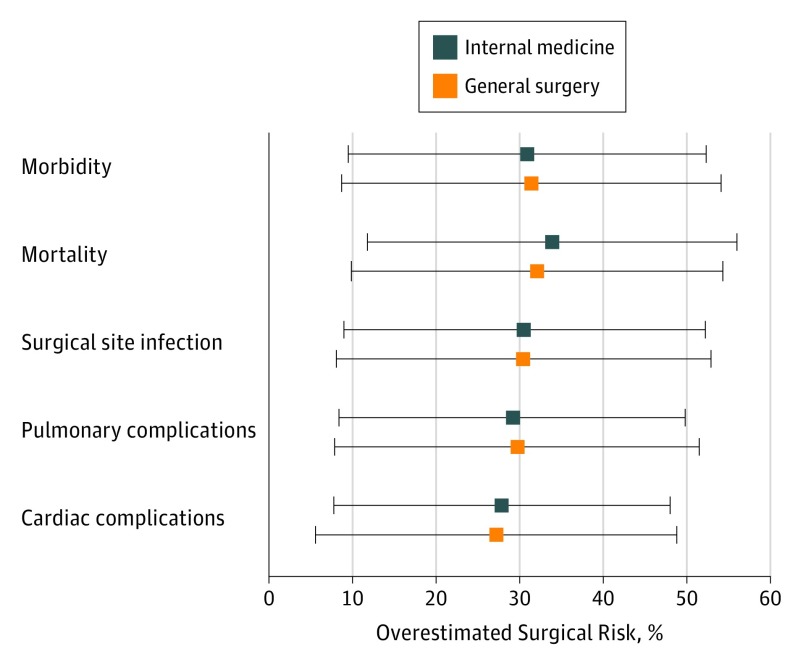
Design, Setting, and Participants: General surgery and internal medicine residents (urban, tertiary, and academic medical center) answered an anonymous, online assessment of 7 real-life, complex clinical scenarios. Participants estimated the chance of any morbidity, mortality, surgical site infection, pneumonia, and cardiac complications. Scenarios represented a diverse general surgery practice, including colectomy, duodenal ulcer repair, inguinal hernia repair, perforated viscus exploration, small-bowel resection, cholecystectomy, and mastectomy in surgically complex patients likely to be comanaged by surgical and internal medicine services.
Main Outcomes and Measures: Responses were compared with risk-adjusted outcomes reported by the American College of Surgeons’ National Surgical Quality Improvement Project (NSQIP) online calculator.
Results: A total of 76 general surgery residents (50 [65.8%] male and 26 [34.2%] female) and 76 internal medicine residents (36 [47.4%] male and 40 [52.6%] female) participated (64% overall response rate). General surgery residents were significantly more confident with their responses (general surgery residents’ mean response, 3.6 [95% CI, 3.4-2.8]; internal medicine residents’ mean response, 2.8 [95% CI, 2.6-3.0]; P < .001) and with not offering operations (general surgery residents’ mean response, 4.3 [95% CI, 4.1-4.4]; internal medicine residents’ mean response, 3.7 [95% CI, 3.4-3.9]; P = .006) but less likely to discuss code status (general surgery residents’ mean response, 3.2 [95% CI, 2.9-3.4]; internal medicine residents’ mean response, 3.8 [95% CI, 3.5-4.1]; P < .001) or consult risk-adjusted models, such as NSQIP (general surgery residents’ mean response, 2.9 [95% CI, 2.7-3.1]; internal medicine residents’ mean response, 3.7 [95% CI, 3.4-4.0]; P < .001). For 91% of clinical estimates, both groups similarly overestimated every type of risk; in 9% of estimates, internal medicine residents had higher overestimates. Estimates varied significantly, with wide 95% CIs; however, only 11% of the NSQIP estimates fell within the 95% CIs. Overall, the mean percentages of the estimates ranged from 26% to 33% over NSQIP estimates for all complications.
Conclusions and Relevance: General surgery and internal medicine residents demonstrated similar estimates of postoperative complications and death. Both groups overestimated risks in surgically complex patient scenarios compared with NSQIP risk calculator estimates. This near-universal overestimation of risk underscores the importance of developing risk-estimation resources for internists and surgeons.
Conflict of interest statement
Figures
Comment in
-
Risk, Complexity, Decision Making, and Patient Care.JAMA Surg. 2018 Mar 1;153(3):208. doi: 10.1001/jamasurg.2017.3930. JAMA Surg. 2018. PMID: 29049428 No abstract available.
Similar articles
-
Management of adverse surgical events: a structured education module for residents.Am J Surg. 2005 Nov;190(5):687-90. doi: 10.1016/j.amjsurg.2005.07.003. Am J Surg. 2005. PMID: 16226940
-
Internal medicine and general surgery residents' attitudes about the ACGME duty hours regulations: a multicenter study.Acad Med. 2006 Dec;81(12):1052-8. doi: 10.1097/01.ACM.0000246687.03462.59. Acad Med. 2006. PMID: 17122468
-
[Phlebology training of general and digestive tract surgery residents (MIR)].Cir Esp. 2010 Aug;88(2):133-4; author reply 134. doi: 10.1016/j.ciresp.2010.03.048. Epub 2010 Jun 22. Cir Esp. 2010. PMID: 20573340 Spanish. No abstract available.
-
Evaluating Coding Accuracy in General Surgery Residents' Accreditation Council for Graduate Medical Education Procedural Case Logs.J Surg Educ. 2016 Nov-Dec;73(6):e59-e63. doi: 10.1016/j.jsurg.2016.07.017. J Surg Educ. 2016. PMID: 27886974 Review.
-
The future of residents' education in internal medicine.Am J Med. 2004 May 1;116(9):648-50. doi: 10.1016/j.amjmed.2004.02.015. Am J Med. 2004. PMID: 15093769 Review. No abstract available.
Cited by
-
Challenges and Solutions in Postoperative Complications: A Narrative Review in General Surgery.Cureus. 2023 Dec 22;15(12):e50942. doi: 10.7759/cureus.50942. eCollection 2023 Dec. Cureus. 2023. PMID: 38264378 Free PMC article. Review.
-
Learning from experience: a qualitative study of surgeons' perspectives on reporting and dealing with serious adverse events.BMJ Open Qual. 2023 Jun;12(2):e002368. doi: 10.1136/bmjoq-2023-002368. BMJ Open Qual. 2023. PMID: 37286299 Free PMC article.
-
An Argument in Favor of Deep Brain Stimulation for Uncommon Movement Disorders: The Case for N-of-1 Trials in Holmes Tremor.Front Hum Neurosci. 2022 Jun 17;16:921523. doi: 10.3389/fnhum.2022.921523. eCollection 2022. Front Hum Neurosci. 2022. PMID: 35782038 Free PMC article.
-
Estimating Surgical Risk for Patients With Severe Comorbidities.JAMA Surg. 2018 Aug 1;153(8):778-780. doi: 10.1001/jamasurg.2018.1055. JAMA Surg. 2018. PMID: 29847676 Free PMC article.
-
Eye of the beholder: Risk calculators and barriers to adoption in surgical trainees.Surgery. 2018 Nov;164(5):1117-1123. doi: 10.1016/j.surg.2018.07.002. Epub 2018 Aug 24. Surgery. 2018. PMID: 30149939 Free PMC article.
References
-
- Albisser Schleger H, Oehninger NR, Reiter-Theil S. Avoiding bias in medical ethical decision-making: lessons to be learnt from psychology research. Med Health Care Philos. 2011;14(2):155-162. - PubMed
-
- McDermott R. Medical decision making: lessons from psychology. Urol Oncol. 2008;26(6):665-668. - PubMed
-
- Sjoberg L. Factors in risk perception. Risk Anal. 2000;20(1):1-11. - PubMed
-
- Fleisher LA. Preoperative assessment of the patient with cardiac disease undergoing noncardiac surgery. Anesthesiol Clin. 2016;34(1):59-70. - PubMed
-
- Chaudhry W, Cohen MC. Cardiac screening in the noncardiac surgery patient. Surg Clin North Am. 2017;97(4):717-732. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
