

Effectiveness of Injectable Extended-Release Naltrexone vs Daily Buprenorphine-Naloxone for Opioid Dependence: A Randomized Clinical Noninferiority Trial
- PMID: 29049469
- PMCID: PMC6583381
- DOI: 10.1001/jamapsychiatry.2017.3206
Effectiveness of Injectable Extended-Release Naltrexone vs Daily Buprenorphine-Naloxone for Opioid Dependence: A Randomized Clinical Noninferiority Trial
Erratum in
-
Error in Introduction.JAMA Psychiatry. 2018 May;75(5):530. doi: 10.1001/jamapsychiatry.2018.0238. Epub 2018 Mar 14. JAMA Psychiatry. 2018. PMID: 29541742 Free PMC article. No abstract available.
Abstract
Importance: To date, extended-release naltrexone hydrochloride has not previously been compared directly with opioid medication treatment (OMT), currently the most commonly prescribed treatment for opioid dependence.
Objective: To determine whether treatment with extended-release naltrexone will be as effective as daily buprenorphine hydrochloride with naloxone hydrochloride in maintaining abstinence from heroin and other illicit substances in newly detoxified individuals.
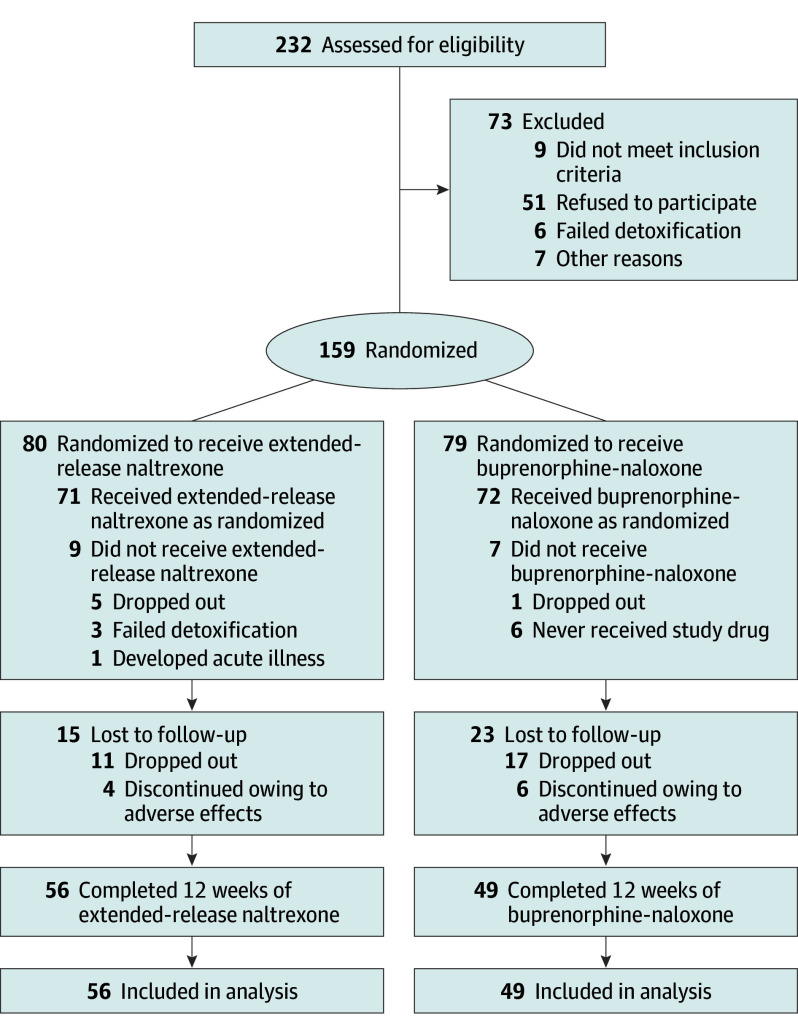
Design, setting and participants: A 12-week, multicenter, outpatient, open-label randomized clinical trial was conducted at 5 urban addiction clinics in Norway between November 1, 2012, and December 23, 2015; the last follow-up was performed on October 23, 2015. A total of 232 adult opioid-dependent (per DSM-IV criteria) individuals were recruited from outpatient addiction clinics and detoxification units and assessed for eligibility. Intention-to-treat analyses of efficacy end points were performed with all randomized participants.
Interventions: Randomization to either daily oral flexible dose buprenorphine-naloxone, 4 to 24 mg/d, or extended-release naltrexone hydrochloride, 380 mg, administered intramuscularly every fourth week for 12 weeks.
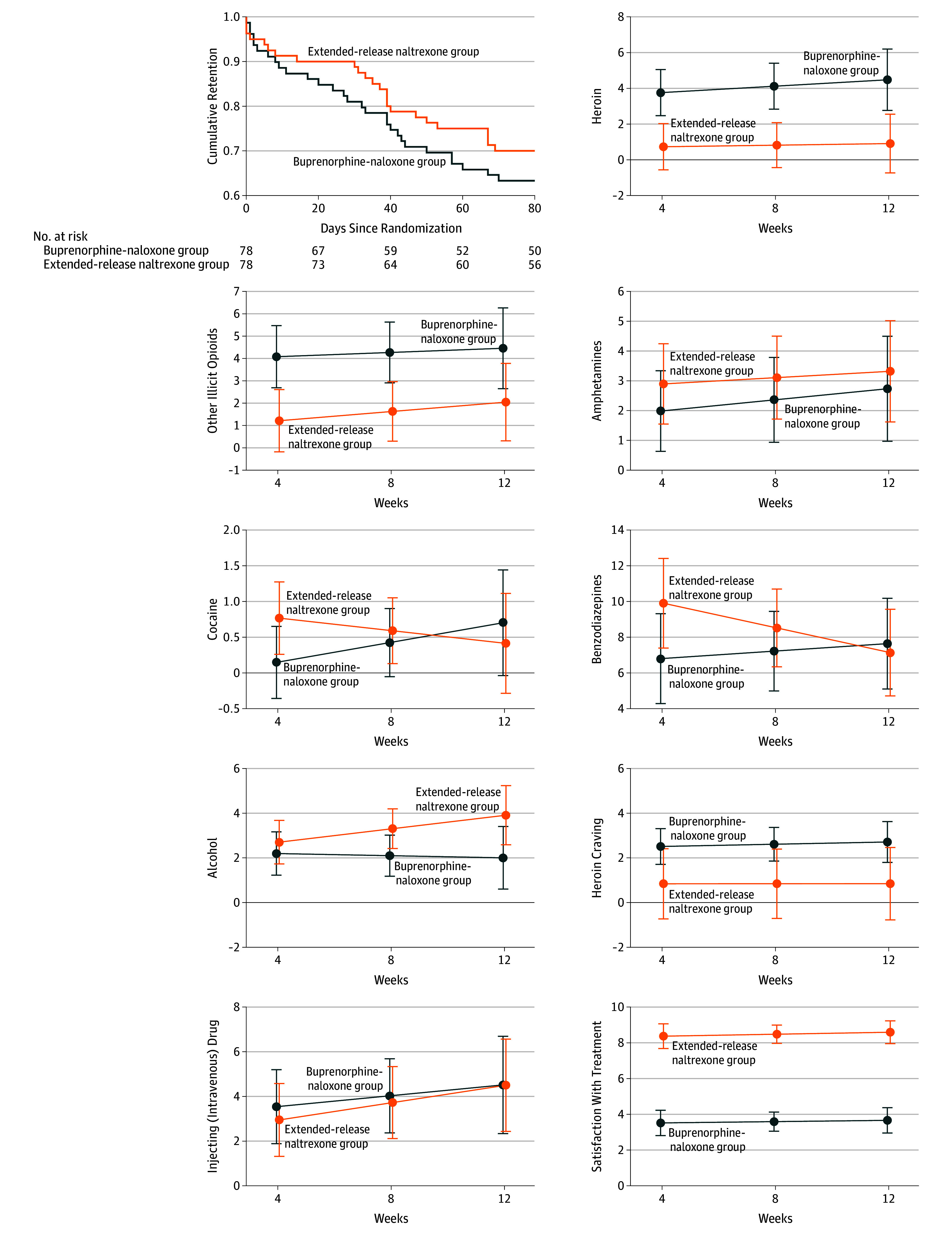
Main outcomes and measures: Primary end points (protocol) were the randomized clinical trial completion rate, the proportion of opioid-negative urine drug tests, and number of days of use of heroin and other illicit opioids. Secondary end points included number of days of use of other illicit substances. Safety was assessed by adverse event reporting.
Results: Of 159 participants, mean (SD) age was 36 (8.6) years and 44 (27.7%) were women. Eighty individuals were randomized to extended-release naltrexone and 79 to buprenorphine-naloxone; 105 (66.0%) completed the trial. Retention in the extended-release naltrexone group was noninferior to the buprenorphine-naloxone group (difference, -0.1; with 95% CI, -0.2 to 0.1; P = .04), with mean (SD) time of 69.3 (25.9) and 63.7 (29.9) days, correspondingly (P = .33, log-rank test). Treatment with extended-release naltrexone showed noninferiority to buprenorphine-naloxone on group proportion of total number of opioid-negative urine drug tests (mean [SD], 0.9 [0.3] and 0.8 [0.4], respectively, difference, 0.1 with 95% CI, -0.04 to 0.2; P < .001) and use of heroin (mean difference, -3.2 with 95% CI, -4.9 to -1.5; P < .001) and other illicit opioids (mean difference, -2.7 with 95% CI, -4.6 to -0.9; P < .001). Superiority analysis showed significantly lower use of heroin and other illicit opioids in the extended-release naltrexone group. No significant differences were found between the treatment groups regarding most other illicit substance use.
Conclusions and relevance: Extended-release naltrexone was as effective as buprenorphine-naloxone in maintaining short-term abstinence from heroin and other illicit substances and should be considered as a treatment option for opioid-dependent individuals.
Trial registration: clinicaltrials.gov Identifier: NCT01717963.
Conflict of interest statement
Figures
References
-
- Volkow ND, Frieden TR, Hyde PS, Cha SS. Medication-assisted therapies—tackling the opioid-overdose epidemic. N Engl J Med. 2014;370(22):2063-2066. - PubMed
-
- McLellan AT, Lewis DC, O’Brien CP, Kleber HD. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284(13):1689-1695. - PubMed
-
- Dole VP, Nyswander M. A medical treatment for diacetylmorphine (heroin) addiction: a clinical trial with methadone hydrochloride. JAMA. 1965;193:646-650. - PubMed
-
- Guidelines for the Psychosocially Assisted Pharmacological Treatment of Opioid Dependence. Geneva, Switzerland: World Health Organization; 2009. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
