

Time Requirements for Electronic Health Record Use in an Academic Ophthalmology Center
- PMID: 29049512
- PMCID: PMC5710390
- DOI: 10.1001/jamaophthalmol.2017.4187
Time Requirements for Electronic Health Record Use in an Academic Ophthalmology Center
Abstract
Importance: Electronic health record (EHR) systems have transformed the practice of medicine. However, physicians have raised concerns that EHR time requirements have negatively affected their productivity. Meanwhile, evolving approaches toward physician reimbursement will require additional documentation to measure quality and cost of care. To date, little quantitative analysis has rigorously studied these topics.
Objective: To examine ophthalmologist time requirements for EHR use.
Design, setting, and participants: A single-center cohort study was conducted between September 1, 2013, and December 31, 2016, among 27 stable departmental ophthalmologists (defined as attending ophthalmologists who worked at the study institution for ≥6 months before and after the study period). Ophthalmologists who did not have a standard clinical practice or who did not use the EHR were excluded.
Exposures: Time stamps from the medical record and EHR audit log were analyzed to measure the length of time required by ophthalmologists for EHR use. Ophthalmologists underwent manual time-motion observation to measure the length of time spent directly with patients on the following 3 activities: EHR use, conversation, and examination.
Main outcomes and measures: The study outcomes were time spent by ophthalmologists directly with patients on EHR use, conversation, and examination as well as total time required by ophthalmologists for EHR use.
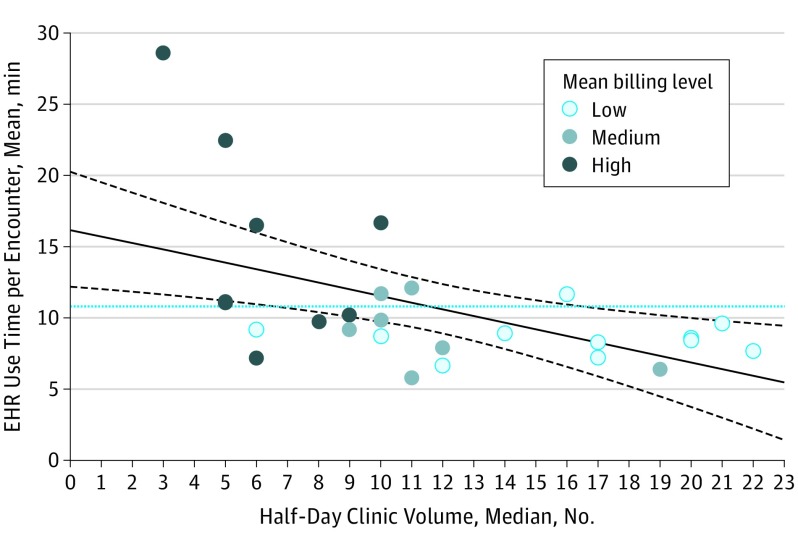
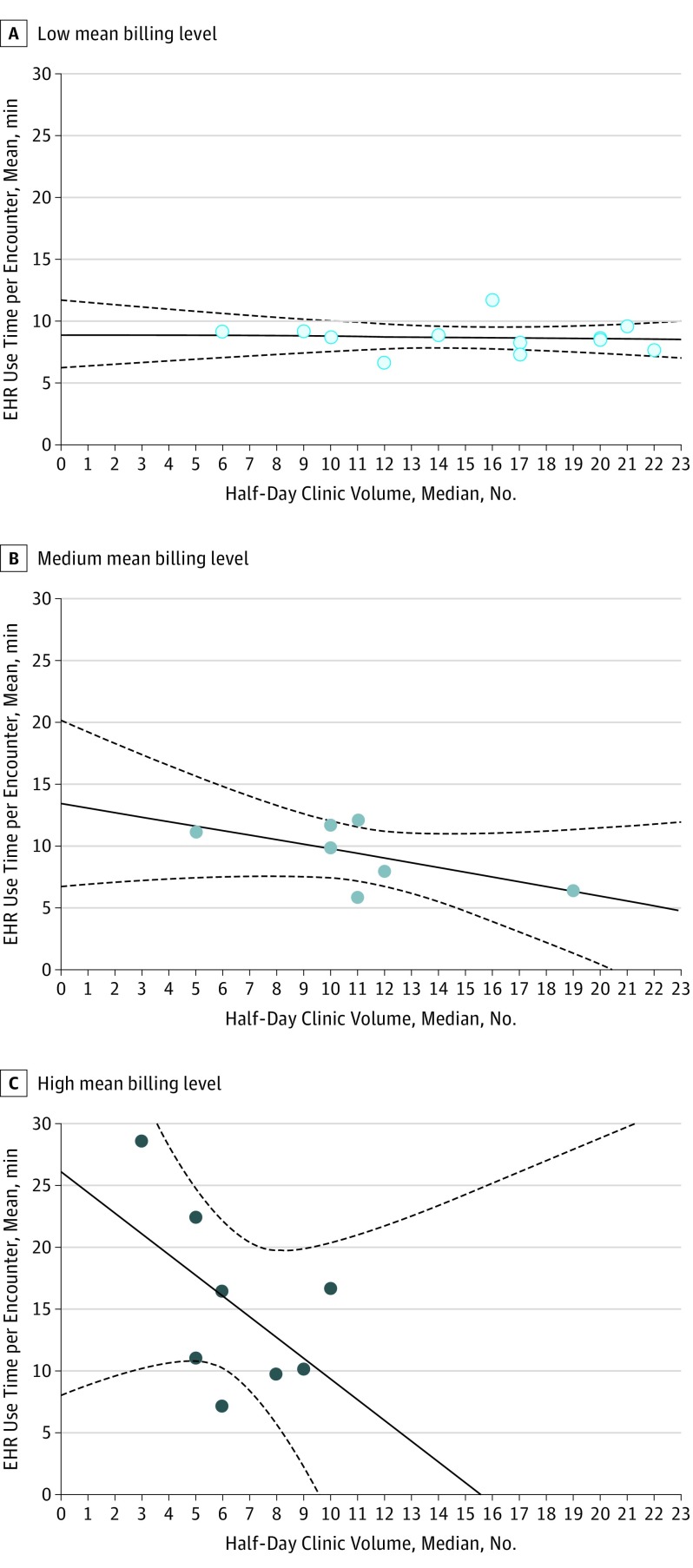
Results: Among the 27 ophthalmologists in this study (10 women and 17 men; mean [SD] age, 47.3 [10.7] years [median, 44; range, 34-73 years]) the mean (SD) total ophthalmologist examination time was 11.2 (6.3) minutes per patient, of which 3.0 (1.8) minutes (27% of the examination time) were spent on EHR use, 4.7 (4.2) minutes (42%) on conversation, and 3.5 (2.3) minutes (31%) on examination. Mean (SD) total ophthalmologist time spent using the EHR was 10.8 (5.0) minutes per encounter (range, 5.8-28.6 minutes). The typical ophthalmologist spent 3.7 hours using the EHR for a full day of clinic: 2.1 hours during examinations and 1.6 hours outside the clinic session. Linear mixed effects models showed a positive association between EHR use and billing level and a negative association between EHR use per encounter and clinic volume. Each additional encounter per clinic was associated with a decrease of 1.7 minutes (95% CI, -4.3 to 1.0) of EHR use time per encounter for ophthalmologists with high mean billing levels (adjusted R2 = 0.42; P = .01).
Conclusions and relevance: Ophthalmologists have limited time with patients during office visits, and EHR use requires a substantial portion of that time. There is variability in EHR use patterns among ophthalmologists.
Conflict of interest statement
Figures
Comment in
-
How Much Time Should We Be Spending With Electronic Health Records?JAMA Ophthalmol. 2017 Nov 1;135(11):1257-1258. doi: 10.1001/jamaophthalmol.2017.3517. JAMA Ophthalmol. 2017. PMID: 29049427 No abstract available.
References
-
- Committee on Improving the Patient Record, Division of Health Care Services, Institute of Medicine The Computer-Based Patient Record: An Essential Technology for Health Care. Revised edition Washington, DC: National Academies Press; 1997. - PubMed
-
- Blumenthal D. Implementation of the federal health information technology initiative. N Engl J Med. 2011;365(25):2426-2431. - PubMed
-
- Jamoom EW, Yang N, Hing E. Adoption of certified electronic health record systems and electronic information sharing in physician offices: United States, 2013 and 2014. NCHS Data Brief. 2016; (236):1-8. - PubMed
-
- Henry J, Pylpchuck Y, Searcy T, Patel V. Adoption of Electronic Health Record Systems Among US Non-Federal Acute Care Hospitals: 2008-2015. Washington, DC: Office of the National Coordinator for Health Information Technology; 2016. ONC Data Brief, No. 35.
-
- Verdon DR. (Slideshow) Medical Economics EHR survey probes physician angst about adoption, use of technology. http://medicaleconomics.modernmedicine.com/medical-economics/content/tag.... Published February 10, 2014. Accessed May 17, 2016.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
