

Comparison of Clinical Characteristics and Outcomes of Peripartum Cardiomyopathy Between African American and Non-African American Women
- PMID: 29049825
- PMCID: PMC5815055
- DOI: 10.1001/jamacardio.2017.3574
Comparison of Clinical Characteristics and Outcomes of Peripartum Cardiomyopathy Between African American and Non-African American Women
Abstract
Importance: Peripartum cardiomyopathy (PPCM) disproportionately affects women of African ancestry, but well-powered studies to explore differences in severity of disease and clinical outcomes are lacking.
Objective: To compare the clinical characteristics, presentation, and outcomes of PPCM between African American and non-African American women.
Design, setting, and participants: This retrospective cohort study using data from January 1, 1986, through December 31, 2016, performed at the University of Pennsylvania Health System, a tertiary referral center serving a population with a high proportion of African American individuals, included 220 women with PPCM.
Main outcomes and measures: Demographic and clinical characteristics and echocardiographic findings at presentation, as well as clinical outcomes including cardiac recovery, time to recovery, cardiac transplant, persistent dysfunction, and death, were compared between African American and non-African American women with PPCM.
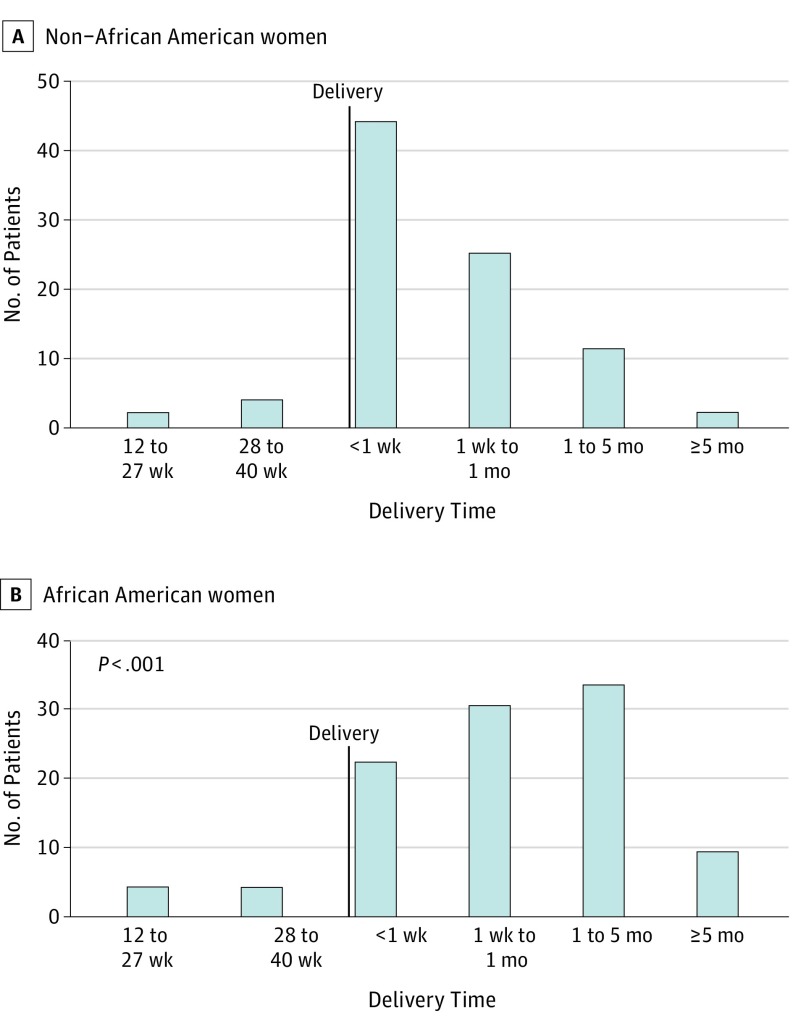
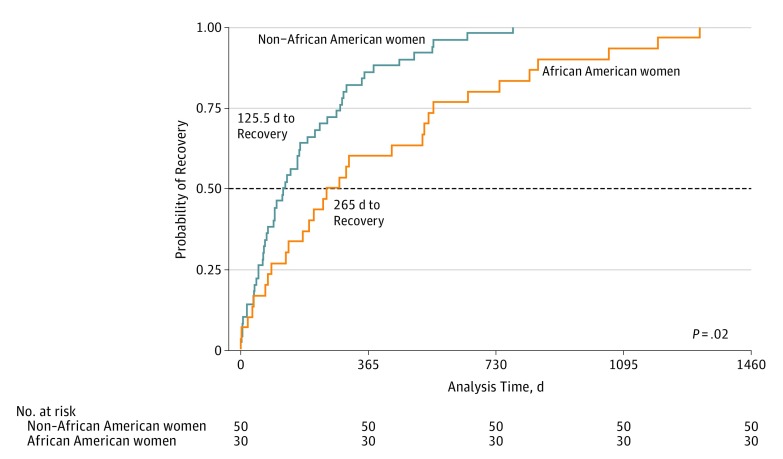
Results: A total of 220 women were studied (mean [SD] age at diagnosis, 29.5 [6.6] years). African American women were diagnosed with PPCM at a younger age (27.6 vs 31.7 years, P < .001), were diagnosed with PPCM later in the postpartum period, and were more likely to present with a left ventricular ejection fraction less than 30% compared with non-African American women (48 [56.5%] vs 30 [39.5%], P = .03). African American women were also more likely to worsen after initial diagnosis (30 [35.3%] vs 14 [18.4%], P = .02), were twice as likely to fail to recover (52 [43.0%] vs 24 [24.2%], P = .004), and, when they did recover, recovery took at least twice as long (median, 265 vs 125.5 days; P = .02) despite apparent adequate treatment.
Conclusions and relevance: In a large cohort of women with well-phenotyped PPCM, this study demonstrates a different profile of disease in African American vs non-African American women. Further work is needed to understand to what extent these differences stem from genetic or socioeconomic differences and how treatment of African American patients might be tailored to improve health outcomes.
Conflict of interest statement
Figures
Comment in
-
Poor Outcomes in Poor Patients?: Peripartum Cardiomyopathy-Not Just Black and White.JAMA Cardiol. 2017 Nov 1;2(11):1261-1262. doi: 10.1001/jamacardio.2017.3605. JAMA Cardiol. 2017. PMID: 29049487 No abstract available.
References
-
- Sliwa K, Hilfiker-Kleiner D, Petrie MC, et al. ; Heart Failure Association of the European Society of Cardiology Working Group on Peripartum Cardiomyopathy . Current state of knowledge on aetiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. Eur J Heart Fail. 2010;12(8):767-778. - PubMed
-
- Arany Z, Elkayam U. Peripartum cardiomyopathy. Circulation. 2016;133(14):1397-1409. - PubMed
-
- Pearson GD, Veille JC, Rahimtoola S, et al. . Peripartum cardiomyopathy: National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) workshop recommendations and review. JAMA. 2000;283(9):1183-1188. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
