

Nationwide Trends in Hospital Outcomes and Utilization After Lower Limb Revascularization in Patients on Hemodialysis
- PMID: 29050629
- PMCID: PMC5685672
- DOI: 10.1016/j.jcin.2017.05.050
Nationwide Trends in Hospital Outcomes and Utilization After Lower Limb Revascularization in Patients on Hemodialysis
Abstract
Objectives: This study aimed to describe the temporal trends and outcomes of endovascular and surgical revascularization in a large, nationally representative sample of patients with end-stage renal disease on hemodialysis hospitalized for peripheral artery disease (PAD).
Background: PAD is prevalent among patients with end-stage renal disease on hemodialysis and is associated with significant morbidity and mortality. There is a paucity of information on trends in endovascular and surgical revascularization and post-procedure outcomes in this population.
Methods: We used the Nationwide Inpatient Sample (2002 to 2012) to identify hemodialysis patients undergoing endovascular or surgical procedures for PAD using diagnostic and procedural codes. We compared trends in amputation, post-procedure complications, mortality, length of stay, and costs between the 2 groups using trend tests and logistic regression.
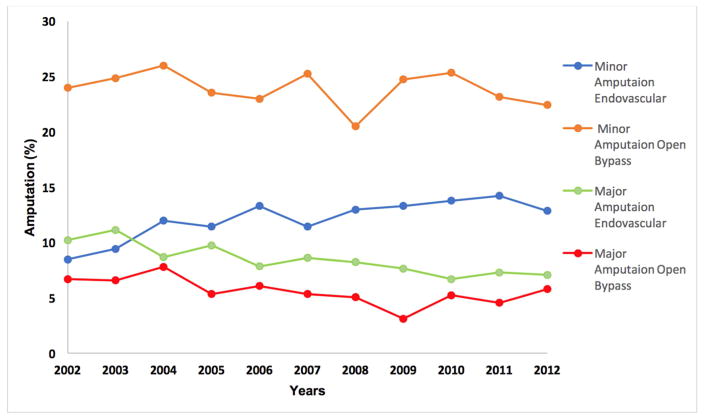
Results: There were 77,049 endovascular and 29,556 surgical procedures for PAD in hemodialysis patients. Trend analysis showed that endovascular procedures increased by nearly 3-fold, whereas there was a reciprocal decrease in surgical revascularization. Post-procedure complication rates were relatively stable in persons undergoing endovascular procedures but nearly doubled in those undergoing surgery. Surgery was associated with 1.8 times adjusted odds (95% confidence interval: 1.60 to 2.02) for complications and 1.6 times the adjusted odds for amputations (95% confidence interval: 1.40 to 1.75) but had similar mortality (adjusted odds ratio: 1.05; 95% confidence interval: 0.85 to 1.29) compared with endovascular procedures. Length of stay for endovascular procedures remained stable, whereas a decrease was seen for surgical procedures. Overall costs increased marginally for both procedures.
Conclusions: Rates of endovascular procedures have increased, whereas those of surgeries have decreased. Surgical revascularization is associated with higher odds of overall complications. Further prospective studies and clinical trials are required to analyze the relationship between the severity of PAD and the revascularization strategy chosen.
Keywords: hemodialysis; peripheral artery disease; revascularization procedures.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures






Comment in
-
Trends in Lower Limb Revascularization Among Patients With End-Stage Renal Failure: Where Is the Journey Going, and How Far Have We Come?JACC Cardiovasc Interv. 2017 Oct 23;10(20):2111-2112. doi: 10.1016/j.jcin.2017.06.061. JACC Cardiovasc Interv. 2017. PMID: 29050630 No abstract available.
Similar articles
-
Trends in hospital treatments for peripheral arterial disease in the United States and association between payer status and quality of care/outcomes, 2007-2011.Catheter Cardiovasc Interv. 2015 Nov;86(5):864-72. doi: 10.1002/ccd.26065. Epub 2015 Oct 8. Catheter Cardiovasc Interv. 2015. PMID: 26446891
-
Trends in Procedure Type, Morbidity and In-Hospital Outcomes of Patients with Peripheral Artery Disease: Data from the Brazilian Public Health System.Ann Vasc Surg. 2016 Feb;31:143-51. doi: 10.1016/j.avsg.2015.08.019. Epub 2015 Nov 23. Ann Vasc Surg. 2016. PMID: 26616503
-
Emerging trends in nationwide mortality, limb loss, and resource utilization for critical limb ischemia in young adults.Cardiovasc Revasc Med. 2024 Oct;67:41-48. doi: 10.1016/j.carrev.2024.04.012. Epub 2024 Apr 14. Cardiovasc Revasc Med. 2024. PMID: 38616461
-
Effects of dialysis on peripheral arterial disease.Semin Vasc Surg. 2024 Dec;37(4):412-418. doi: 10.1053/j.semvascsurg.2024.09.001. Epub 2024 Oct 5. Semin Vasc Surg. 2024. PMID: 39675850 Review.
-
End-stage renal disease and limb salvage.Methodist Debakey Cardiovasc J. 2013 Apr;9(2):108-11. doi: 10.14797/mdcj-9-2-108. Methodist Debakey Cardiovasc J. 2013. PMID: 23805345 Free PMC article. Review.
Cited by
-
Cell Therapy of Severe Ischemia in People with Diabetic Foot Ulcers-Do We Have Enough Evidence?Mol Diagn Ther. 2023 Nov;27(6):673-683. doi: 10.1007/s40291-023-00667-w. Epub 2023 Sep 22. Mol Diagn Ther. 2023. PMID: 37740111 Free PMC article.
-
Systemic outcomes of symptomatic peripheral artery disease patients with end-stage renal disease undergoing lower limb endovascular treatment: a propensity score-matched analysis.BMC Cardiovasc Disord. 2025 May 21;25(1):388. doi: 10.1186/s12872-025-04838-x. BMC Cardiovasc Disord. 2025. PMID: 40394492 Free PMC article.
-
Major Lower Limb Amputations and Amputees in an Aging Population in Southwest Finland 2007-2017.Clin Interv Aging. 2022 Jun 8;17:925-936. doi: 10.2147/CIA.S361547. eCollection 2022. Clin Interv Aging. 2022. PMID: 35707730 Free PMC article.
-
Outcomes of Lower Extremity Endovascular Revascularization: Potential Predictors and Prevention Strategies.Int J Mol Sci. 2021 Feb 18;22(4):2002. doi: 10.3390/ijms22042002. Int J Mol Sci. 2021. PMID: 33670461 Free PMC article. Review.
References
-
- O'Hare AM, Feinglass J, Sidawy AN, et al. Impact of renal insufficiency on short-term morbidity and mortality after lower extremity revascularization: data from the Department of Veterans Affairs' National Surgical Quality Improvement Program. J Am Soc Nephrol. 2003;14:1287–95. - PubMed
-
- Rooke TW, Hirsch AT, Misra S, et al. 2011 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Peripheral Artery Disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;58:2020–45. - PMC - PubMed
-
- Agarwal S, Sud K, Shishehbor MH. Nationwide Trends of Hospital Admission and Outcomes Among Critical Limb Ischemia Patients: From 2003–2011. J Am Coll Cardiol. 2016;67:1901–13. - PubMed
-
- O'Hare A, Johansen K. Lower-extremity peripheral arterial disease among patients with end-stage renal disease. Journal of the American Society of Nephrology : JASN. 2001;12:2838–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
