

Health Care Costs Associated with AKI
- PMID: 29051143
- PMCID: PMC5672961
- DOI: 10.2215/CJN.00950117
Health Care Costs Associated with AKI
Abstract
Background and objectives: An understanding of the health care resource use associated with AKI is needed to frame the investment and cost-effectiveness of strategies to prevent AKI and promote kidney recovery.
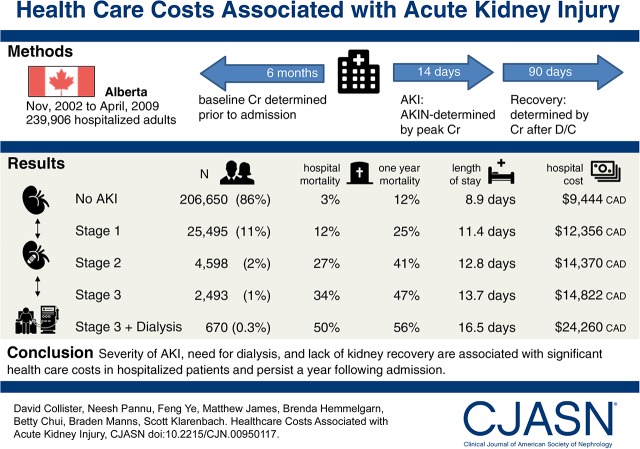
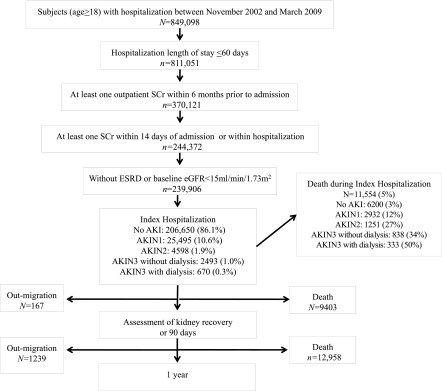
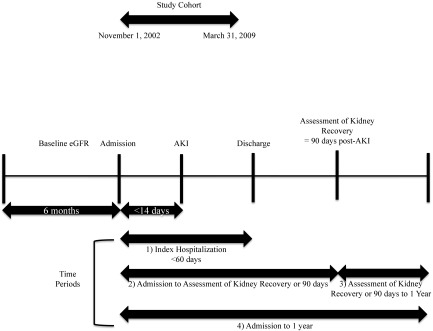
Design, setting, participants, & measurements: We assembled population-based cohort of adults hospitalized in Alberta between November of 2002 and March of 2009 without ESRD or an eGFR<15 ml/min per 1.73 m2. Outpatient serum creatinine measurements 6 months preceding admission defined baseline kidney function, and serum creatinine during the first 14 days of hospitalization defined Acute Kidney Injury Network stage; kidney recovery defined as serum creatinine within 25% of baseline and independence from dialysis was assessed at 90 days after AKI. Health care utilization and costs (in 2015 Canadian dollars) were determined from inpatient, outpatient, and physician claims datasets during the index hospitalization, recovery period (90 days post-AKI assessment), and 3-12 months post-AKI. A fully adjusted generalized linear model regression analysis was used to estimate costs associated with AKI.
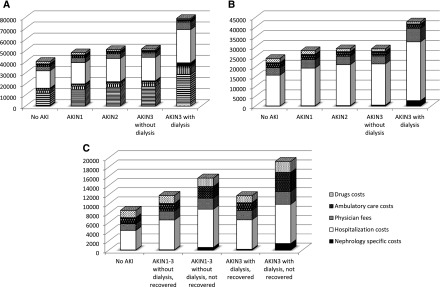
Results: Of 239,906 hospitalized subjects, 25,495 (10.6%), 4598 (1.9%), 2493 (1.0%), and 670 (0.3%) had Acute Kidney Injury Network stages 1, 2, 3 without dialysis, and 3 with dialysis, respectively. Greater severity of AKI was associated with incremental increases in length of stay (+2.8; 95% confidence interval, 1.4 to 4.3 to +7.4; 95% confidence interval, 7.2 to 7.5 days) and costs (+$3779; 95% confidence interval, $3555 to $4004 to +$18,291; 95% confidence interval, $15,573 to $21,009 Canadian dollars) from admission to recovery assessment (3 months). At months 3-12 postadmission, compared with subjects without AKI, AKI with kidney recovery and AKI without kidney recovery were associated with incremental costs of +$2912-$3231 and +$6035-$8563 Canadian dollars, respectively. The estimated incremental cost of AKI in Canada is estimated to be over $200 million Canadian dollars per year.
Conclusions: Severity of AKI, need for dialysis, and lack of kidney recovery are associated with significant health care costs in hospitalized patients and persist a year after admission. Strategies to identify, prevent, and facilitate kidney recovery are needed.
Keywords: Acute Kidney Injury; Alberta; Canada; Cost-Benefit Analysis; Health Care Costs; Inpatients; Investments; Kidney Failure, Chronic; Kidney Function Tests; Length of Stay; Linear Models; Outpatients; Renal Insufficiency, Chronic; acute renal failure; chronic kidney disease; costs; creatinine; dialysis; hospitalization; resource utilization.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Liaño F, Pascual J; Madrid Acute Renal Failure Study Group : Epidemiology of acute renal failure: A prospective, multicenter, community-based study. Kidney Int 50: 811–818, 1996 - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C; Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators : Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 294: 813–818, 2005 - PubMed
-
- Liangos O, Wald R, O’Bell JW, Price L, Pereira BJ, Jaber BL: Epidemiology and outcomes of acute renal failure in hospitalized patients: A national survey. Clin J Am Soc Nephrol 1: 43–51, 2006 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
