

Prediction of recurrence in early stage non-small cell lung cancer using computer extracted nuclear features from digital H&E images
- PMID: 29051570
- PMCID: PMC5648794
- DOI: 10.1038/s41598-017-13773-7
Prediction of recurrence in early stage non-small cell lung cancer using computer extracted nuclear features from digital H&E images
Abstract
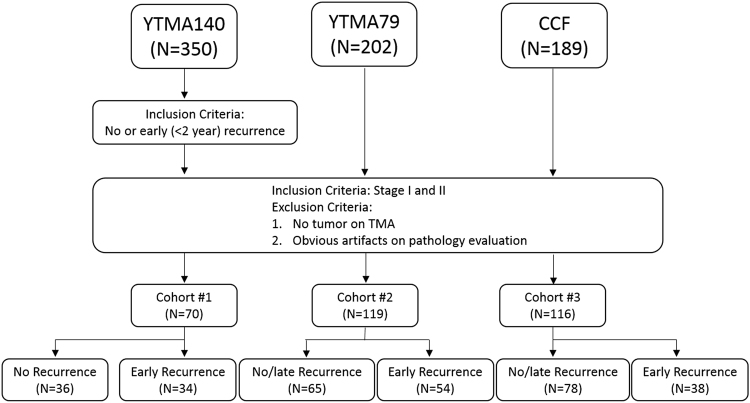
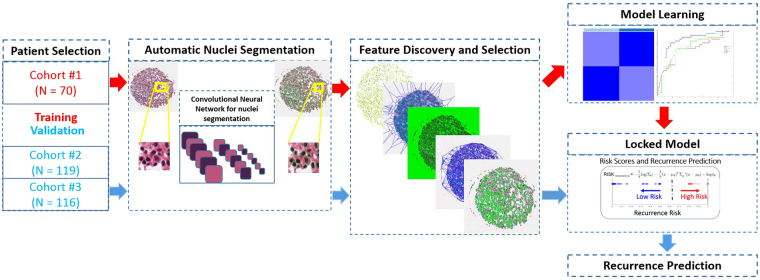
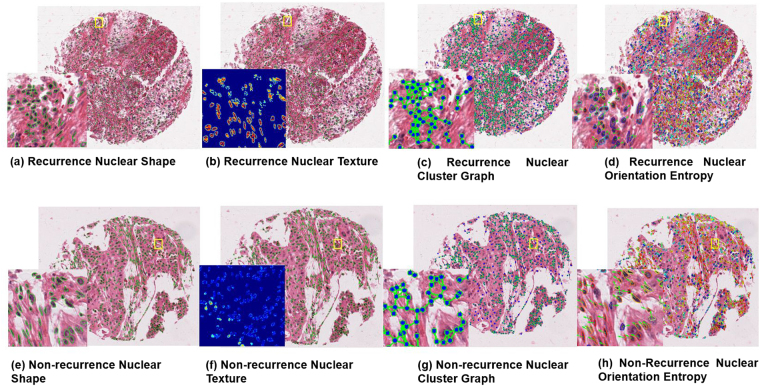
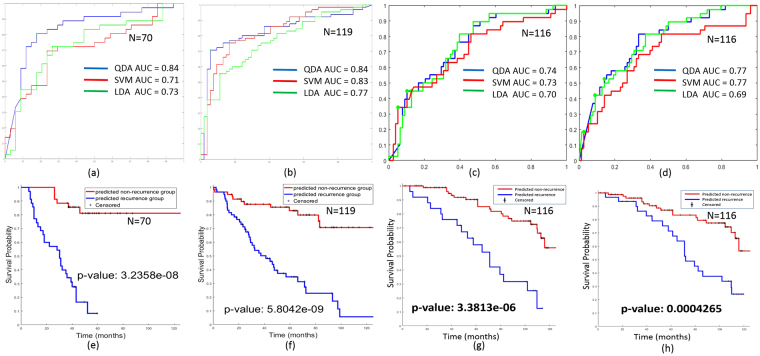
Identification of patients with early stage non-small cell lung cancer (NSCLC) with high risk of recurrence could help identify patients who would receive additional benefit from adjuvant therapy. In this work, we present a computational histomorphometric image classifier using nuclear orientation, texture, shape, and tumor architecture to predict disease recurrence in early stage NSCLC from digitized H&E tissue microarray (TMA) slides. Using a retrospective cohort of early stage NSCLC patients (Cohort #1, n = 70), we constructed a supervised classification model involving the most predictive features associated with disease recurrence. This model was then validated on two independent sets of early stage NSCLC patients, Cohort #2 (n = 119) and Cohort #3 (n = 116). The model yielded an accuracy of 81% for prediction of recurrence in the training Cohort #1, 82% and 75% in the validation Cohorts #2 and #3 respectively. A multivariable Cox proportional hazard model of Cohort #2, incorporating gender and traditional prognostic variables such as nodal status and stage indicated that the computer extracted histomorphometric score was an independent prognostic factor (hazard ratio = 20.81, 95% CI: 6.42-67.52, P < 0.001).
Conflict of interest statement
Xiangxue Wang, Andrew Janowczyk, Yu Zhou, Rajat Thawani and Pingfu Fu have no conflicts to declare. Dr. Schalper is a Consultant for Viralytics. He has received research funding from Genoptix (Novartis), Vasculox, Tesaro, Onkaido Therapeutics and Takeda Pharmaceuticals. Dr. Velcheti is a Consultant for Clovis Oncology, Genertech, Bristol-Myers Squibb, Merck, Celgene, Foundation Medicine, AstraZeneca/MedImmune and Genoptix. He has received research funding from Genentech, Trovagene, Eisai, OncoPlex Diagnostics, Alkermes, NantOmics, Genoptix, Altor BioScience, Merck, Bristol-Myers Squibb, Atreca, Heat Biologics and Leap Therapeutics. Dr. Madabhushi is an equity holder in Elucid Bioimaging and in Inspirata Inc. He is also a scientific advisory consultant for Inspirata Inc and also sits on its scientific advisory board. He is also an equity holder in Inspirata Inc. Additionally his technology has been licensed to Elucid Bioimaging and Inspirata Inc. He is also involved in a NIH U24 grant with PathCore Inc. His work is also partially sponsored by Philips Healthcare.
Figures
References
-
- Laskin, J. J. Adjuvant chemotherapy for non-small cell lung cancer: the new standard of care. (2005). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
