

The Anterolateral Complex of the Knee
- PMID: 29051903
- PMCID: PMC5638167
- DOI: 10.1177/2325967117730805
The Anterolateral Complex of the Knee
Abstract
Background: Significant controversy exists regarding the anterolateral structures of the knee.
Purpose: To determine the layer-by-layer anatomic structure of the anterolateral complex of the knee.
Study design: Descriptive laboratory study.
Methods: Twenty fresh-frozen cadaveric knees (age range, 38-56 years) underwent a layer-by-layer dissection to systematically expose and identify the various structures of the anterolateral complex. Quantitative measurements were performed, and each layer was documented with high-resolution digital imaging.
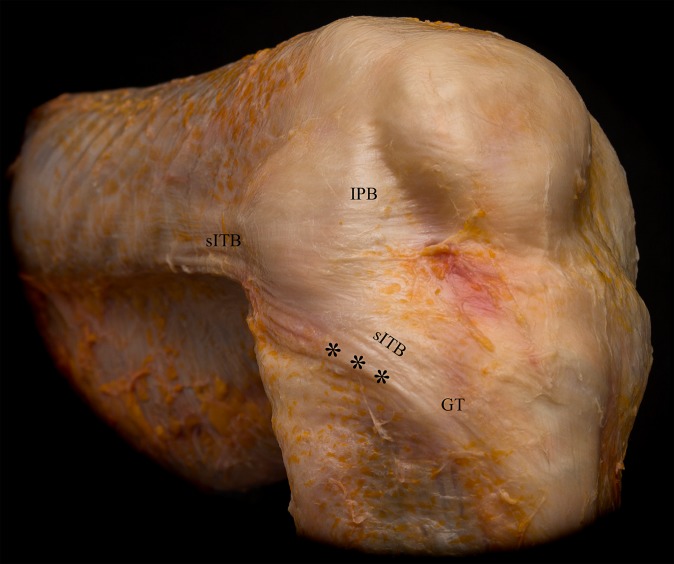
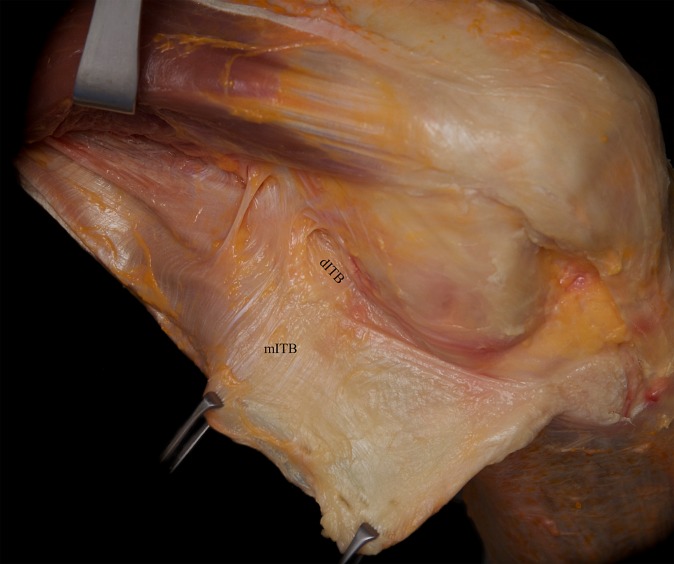
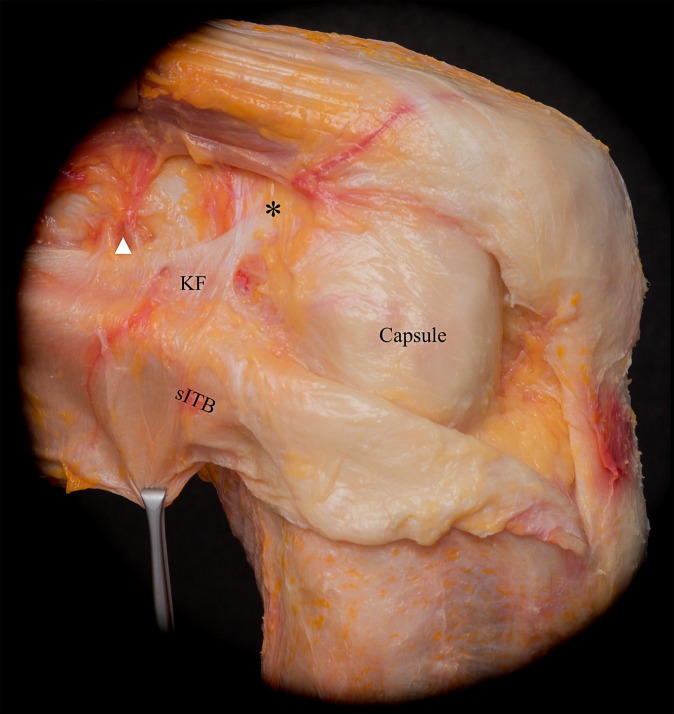
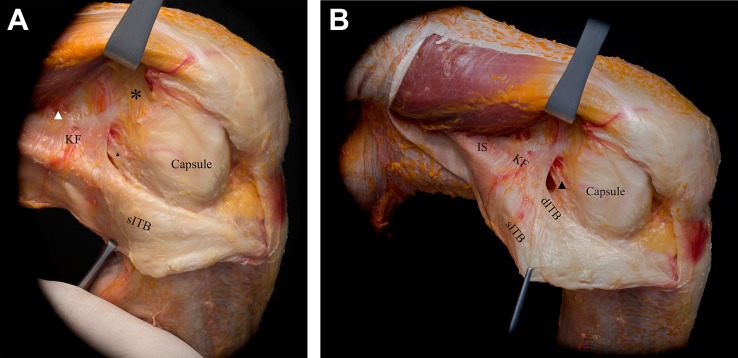
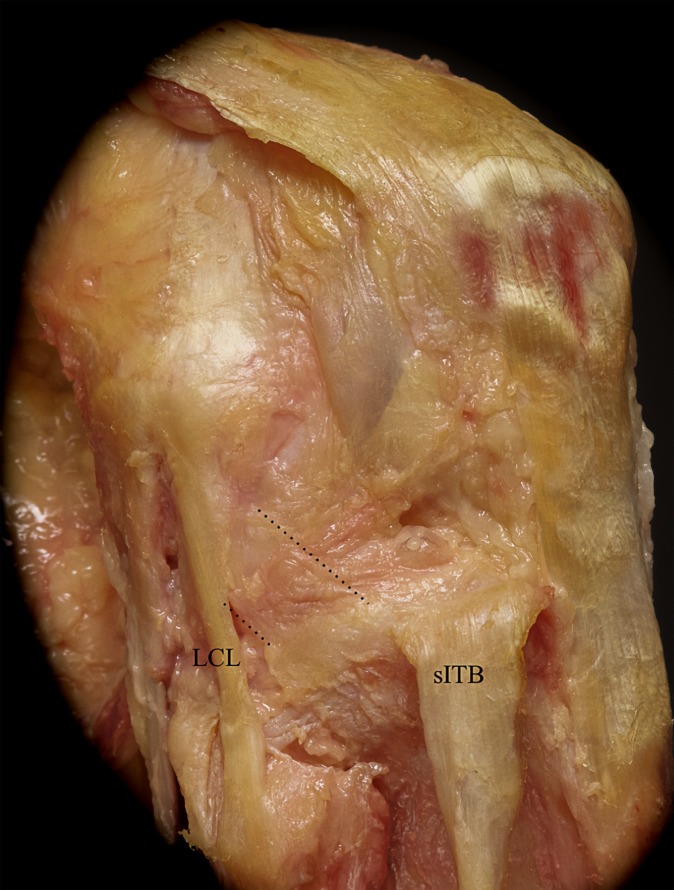
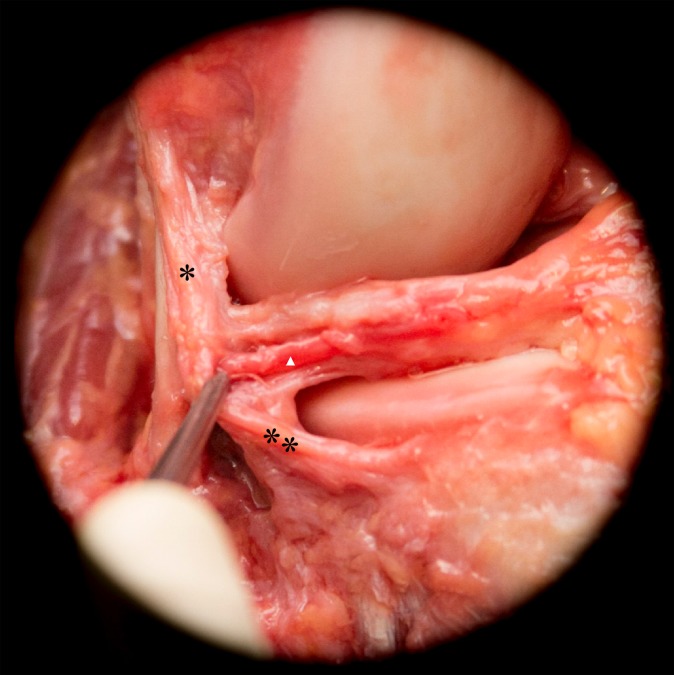
Results: The anterolateral complex of the knee consisted of different distinct layers, with the superficial and deep iliotibial band (ITB) representing layer 1. The superficial ITB had a distinct connection to the distal femoral metaphysis and femoral condyle (Kaplan fibers), and the deep layers of the ITB were identified originating at the level of the Kaplan fibers proximally. This functional unit, consisting of the superficial and deep ITB, was reinforced by the capsulo-osseous layer of the ITB, which was continuous with the fascia of the lateral gastrocnemius and biceps femoris muscles. These 3 components of the ITB became confluent distally, and the insertion spanned from the Gerdy tubercle anteriorly to the lateral tibia posteriorly on a small tubercle (lateral tibial tuberosity). Layer 3 consisted of the anterolateral capsule, in which 35% (7/20) of specimens had a discreet mid-third capsular ligament.
Conclusion: The anterolateral complex consists of the superficial and deep ITB, the capsulo-osseous layer of the ITB, and the anterolateral capsule. The anterolateral complex is defined by the part of the ITB between the Kaplan fibers proximally and its tibial insertion, which forms a functional unit. A discrete anterolateral ligament was not observed; however, the anterolateral ligament described in recent studies likely refers to the capsulo-osseous layer or the mid-third capsular ligament.
Clinical relevance: The anterolateral knee structures form a complex functional unit. Surgeons should use caution when attempting to restore this intricate structure with extra-articular procedures designed to re-create a single discreet ligament.
Keywords: ITB; anatomy; anterolateral; capsule; capsulo-osseous layer; iliotibial band; knee; pivot shift.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Support for this research was received from the Department of Orthopaedic Surgery of the University of Pittsburgh.
Figures

References
-
- Bonanzinga T, Signorelli C, Grassi A, et al. Kinematics of ACL and anterolateral ligament, part I: combined lesion. Knee Surg Sports Traumatol Arthrosc. 2017;25(4):1055–1061. - PubMed
-
- Bull AM, Earnshaw PH, Smith A, Katchburian MV, Hassan AN, Amis AA. Intraoperative measurement of knee kinematics in reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br. 2002;84(7):1075–1081. - PubMed
-
- Caterine S, Litchfield R, Johnson M, Chronik B, Getgood A. A cadaveric study of the anterolateral ligament: re-introducing the lateral capsular ligament. Knee Surg Sports Traumatol Arthrosc. 2015;23(11):3186–3195. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
