

Association of Prognostic Factors and Immunosuppressive Treatment With Long-term Outcomes in Neurosarcoidosis
- PMID: 29052709
- PMCID: PMC5710577
- DOI: 10.1001/jamaneurol.2017.2492
Association of Prognostic Factors and Immunosuppressive Treatment With Long-term Outcomes in Neurosarcoidosis
Abstract
Importance: Prognostic factors are lacking in neurosarcoidosis (NS), and the association of immunosuppressive treatments with outcomes are unclear.
Objectives: To identify prognostic factors of and analyze the association of immunosuppressive treatment with relapse of NS.
Design, setting, and participants: In this retrospective study, a cohort of 234 patients fulfilled the diagnostic criteria for NS in a tertiary referral center in Paris, France, from January 1, 1990, through December 31, 2015. The median follow-up was 8 years (range, 2 months to 23 years).
Main outcomes and measures: All neurologic and extraneurologic data and treatments were analyzed. Functional outcomes measured by the absolute value and the variation from baseline of the Expanded Disability Status Scale (EDSS) score at 60 months after the diagnosis, overall survival, and relapse-free survival (RFS) were assessed. Analyses were stratified by the period of NS diagnosis (1990-1999 vs 2000-2015).
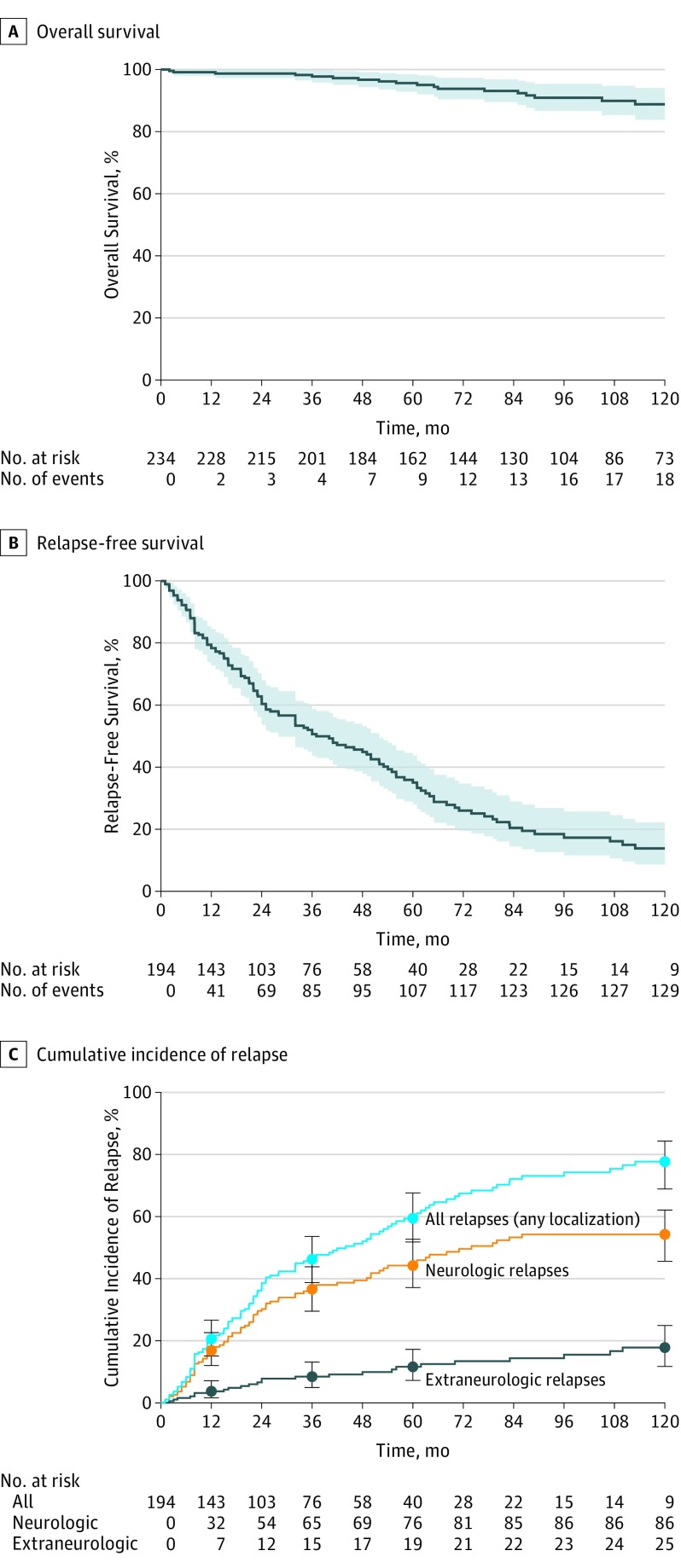
Results: The 234 patients undergoing assessment included 117 women (50.0%) and 117 men (50.0%); median age was 42 years (interquartile range, 32-53 years). The probable 10-year survival rate was 89% (95% CI, 84%-94%). Older age (hazard ratio [HR] per 10 years, 1.64; 95% CI, 1.19-2.27; P = .003), peripheral nervous system involvement (HR, 6.75; 95% CI, 2.31-19.7; P < .001), and higher baseline EDSS score (HR per point, 1.21; 95% CI, 1.06-1.39; P = .005) were associated with mortality. The estimated 10-year RFS rate was 14% (95% CI, 9%-22%) for all relapses and 28% (95% CI, 20%-38%) for neurologic relapses. Encephalic involvement was associated with shorter neurologic RFS (HR, 2.35; 95% CI, 1.44-3.83; P < .001). A lower risk for relapse was associated with cyclophosphamide (HR, 0.26; 95% CI, 0.11-0.59; P = .001), methotrexate sodium (HR, 0.47; 95% CI, 0.25-0.87; P = .02), and infliximab (HR, 0.16; 95% CI, 0.02-1.24; P = .08) treatments. Follow-up was greater than 60 months in 160 patients (68.4%). An elevated baseline EDSS score (odds ratio [OR] per point, 1.92; 95% CI, 1.55-2.37; P < .001), tobacco use (OR, 3.64; 95% CI, 1.36-9.73; P = .01), encephalic symptoms (OR, 3.04; 95% CI, 1.11-8.38; P = .03), and less than 4 extraneurologic sarcoidosis localizations (OR, 3.06; 95% CI, 1.04-8.98; P = .04) were associated with an EDSS value of at least 2.5 at 60 months. Encephalic involvement (16 of 17 patients [94.1%]; P = .008) and peripheral nervous system involvement (5 of 17 patients [29.4%]; P = .03) were associated with worsening of the EDSS score at 60 months.
Conclusions and relevance: This study identifies putative factors affecting morbidity and mortality in patients with NS. Immunosuppressive therapies (ie, intravenous cyclophosphamide, methotrexate, and infliximab) in these patients may be associated with lower relapse rates.
Conflict of interest statement
Figures
Comment in
-
Demystifying Neurosarcoidosis and Informing Prognosis.JAMA Neurol. 2017 Nov 1;74(11):1296-1298. doi: 10.1001/jamaneurol.2017.1473. JAMA Neurol. 2017. PMID: 29052731 No abstract available.
References
-
- Zajicek JP, Scolding NJ, Foster O, et al. Central nervous system sarcoidosis: diagnosis and management. QJM. 1999;92(2):103-117. - PubMed
-
- Chapelon C, Ziza JM, Piette JC, et al. Neurosarcoidosis: signs, course and treatment in 35 confirmed cases. Medicine (Baltimore). 1990;69(5):261-276. - PubMed
-
- Gascón-Bayarri J, Mañá J, Martínez-Yélamos S, Murillo O, Reñé R, Rubio F. Neurosarcoidosis: report of 30 cases and a literature survey. Eur J Intern Med. 2011;22(6):e125-e132. - PubMed
-
- Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an Expanded Disability Status Scale (EDSS). Neurology. 1983;33(11):1444-1452. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
