

Identification of barriers to insulin therapy and approaches to overcoming them
- PMID: 29053215
- PMCID: PMC5836933
- DOI: 10.1111/dom.13132
Identification of barriers to insulin therapy and approaches to overcoming them
Abstract
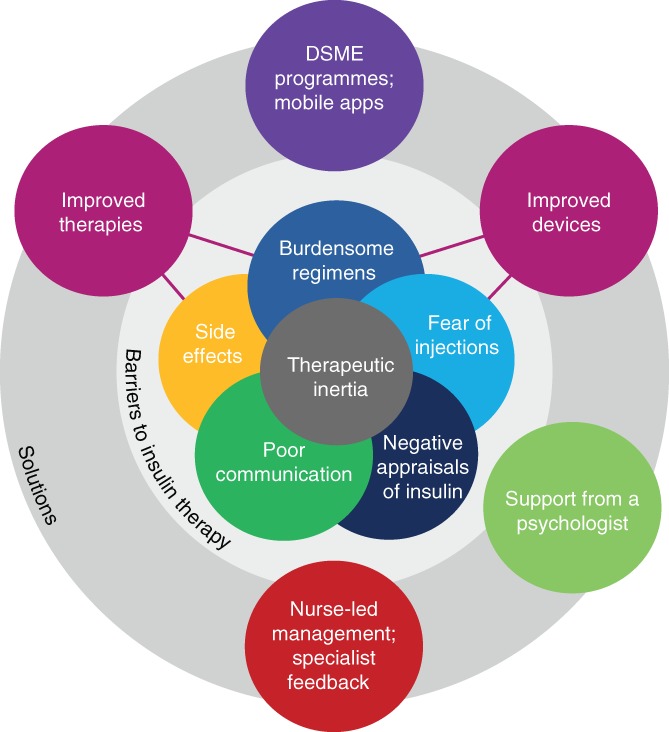
Poor glycaemic control in type 2 diabetes (T2D) is a global problem despite the availability of numerous glucose-lowering therapies and clear guidelines for T2D management. Tackling clinical or therapeutic inertia, where the person with diabetes and/or their healthcare providers do not intensify treatment regimens despite this being appropriate, is key to improving patients' long-term outcomes. This gap between best practice and current level of care is most pronounced when considering insulin regimens, with studies showing that insulin initiation/intensification is frequently and inappropriately delayed for several years. Patient- and physician-related factors both contribute to this resistance at the stages of insulin initiation, titration and intensification, impeding achievement of optimal glycaemic control. The present review evaluates the evidence and reasons for this delay, together with available methods for facilitation of insulin initiation or intensification.
Keywords: insulin therapy; type 2 diabetes.
© 2017 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
D. R. J. reports having received research funds from AstraZeneca, Sanofi‐Aventis, Novo Nordisk, Janssen, Takeda, Boehringer Ingelheim, and speaker honoraria from AstraZeneca, Sanofi‐Aventis, Lilly, Novo Nordisk, Janssen, Takeda and Boehringer Ingelheim, and has been a consultant, board member or member of advisory panels for AstraZeneca, Sanofi‐Aventis, Lilly and Novo Nordisk. F. P. has received research support from Novo Nordisk to analyse data from the DAWN2 study. K. K. reports having received speaker honoraria from Novartis, Novo Nordisk, Sanofi‐Aventis, Lilly, Merck Sharp & Dohme, Janssen, AstraZeneca and Boehringer Ingelheim, and having received research support from Novartis, Novo Nordisk, Sanofi‐Aventis, Lilly, Pfizer, Boehringer Ingelheim, Merck Sharp & Dohme, Janssen and Roche, and being a consultant for Novartis, Novo Nordisk, Sanofi‐Aventis, Lilly, Merck Sharp & Dohme, Janssen, AstraZeneca and Boehringer Ingelheim, and being a member of advisory panels for Lilly, Sanofi‐Aventis, Merck Sharp & Dohme, Novo Nordisk, Boehringer Ingelheim, Janssen, BMS, AstraZeneca, Amgen and Servier.
Figures
References
-
- Fong DS, Aiello LP, Ferris FL III, Klein R. Diabetic retinopathy. Diabetes Care. 2004;27(10):2540–2553. - PubMed
-
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10‐year follow‐up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–1589. - PubMed
-
- Ray KK, Seshasai SR, Wijesuriya S, et al. Effect of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes mellitus: a meta‐analysis of randomised controlled trials. Lancet. 2009;373(9677):1765–1772. - PubMed
-
- Khunti K, Millar‐Jones D. Clinical inertia to insulin initiation and intensification in the UK: a focused literature review. Prim Care Diabetes. 2017;11(1):3–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
