

What Are We Missing? False-Negative Cancers at Multiparametric MR Imaging of the Prostate
- PMID: 29053402
- PMCID: PMC5749595
- DOI: 10.1148/radiol.2017152877
What Are We Missing? False-Negative Cancers at Multiparametric MR Imaging of the Prostate
Abstract
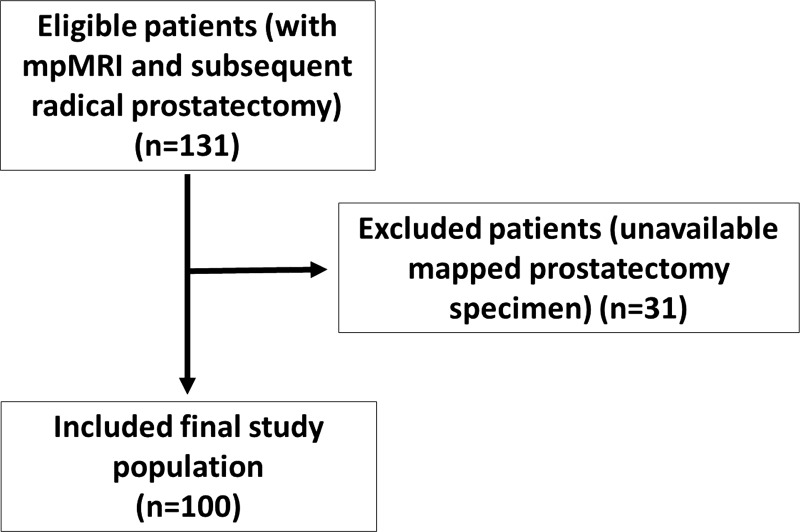
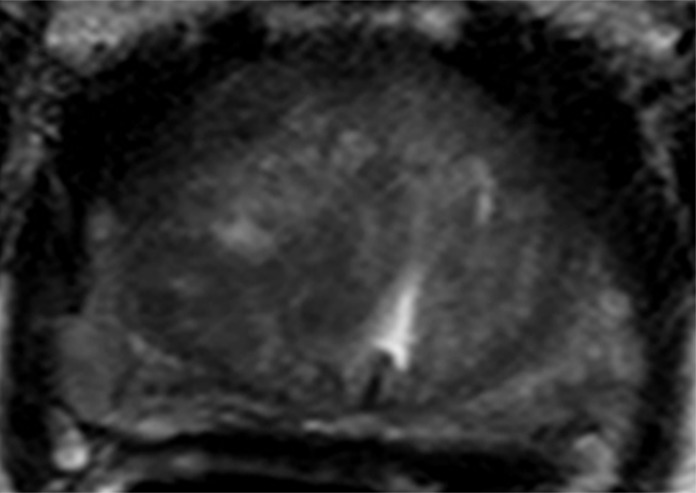
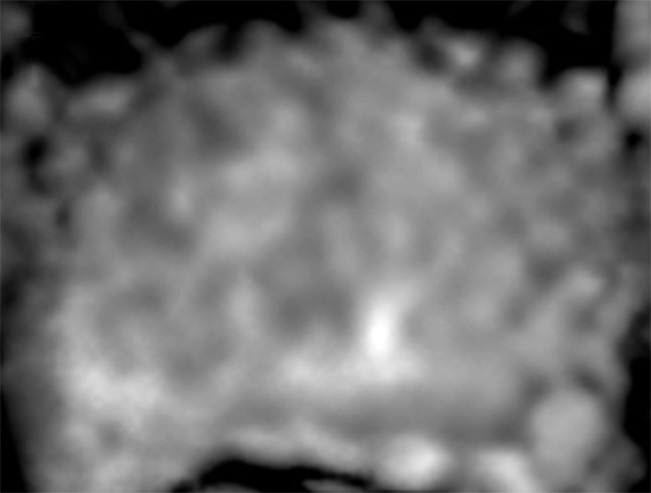
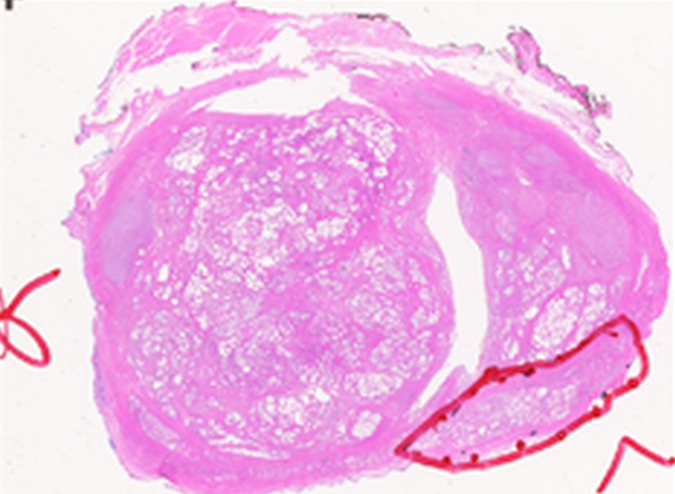
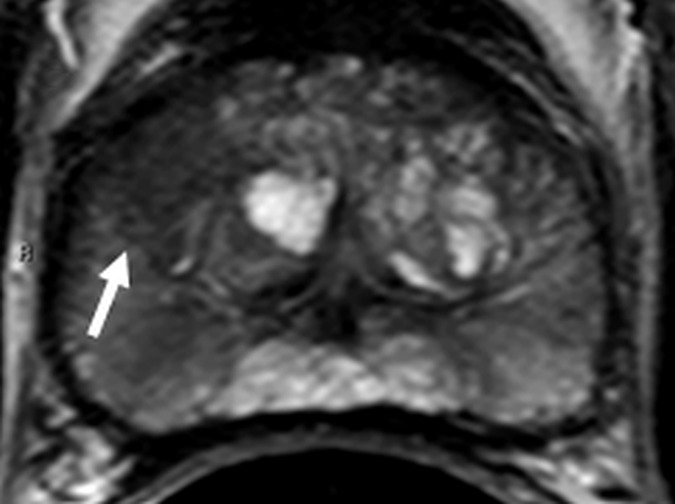
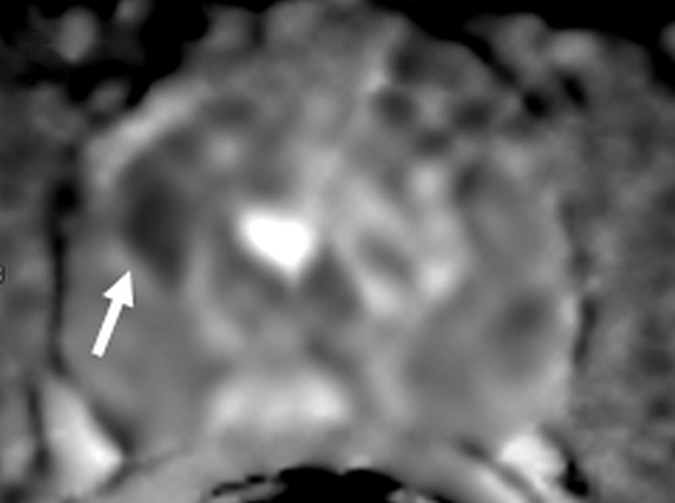
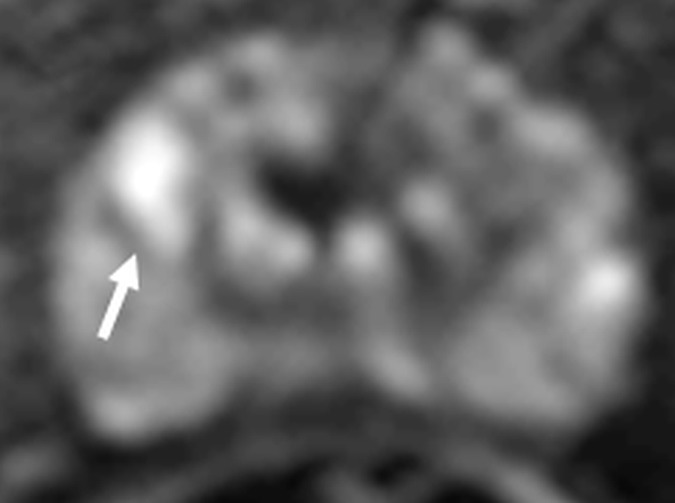
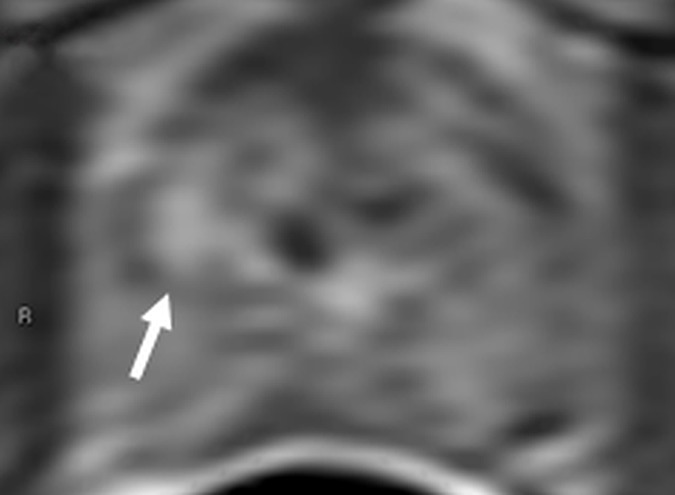
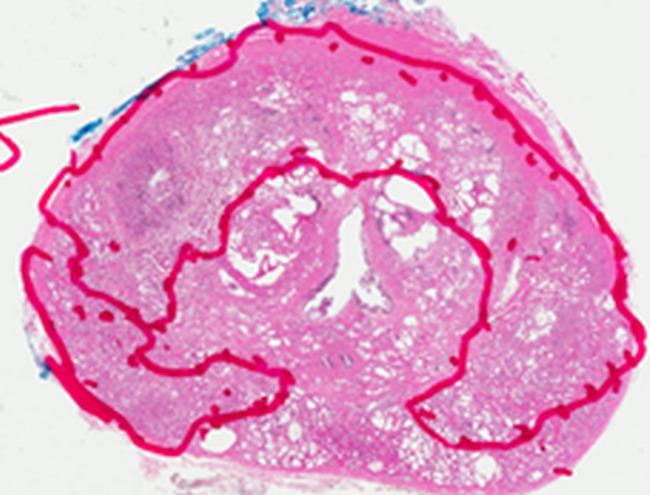
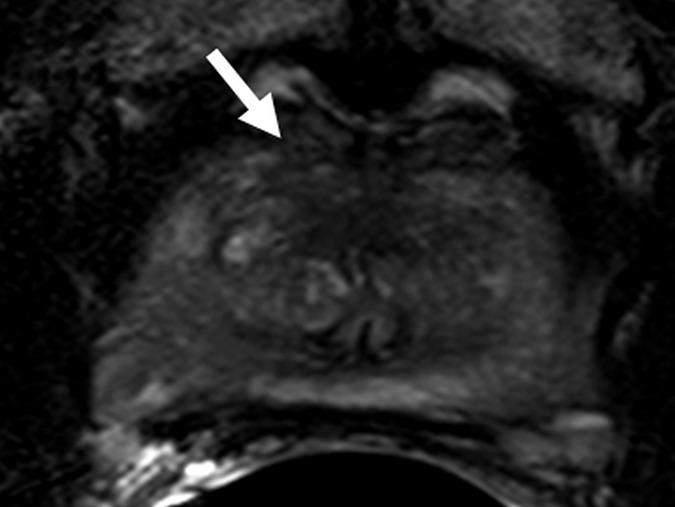
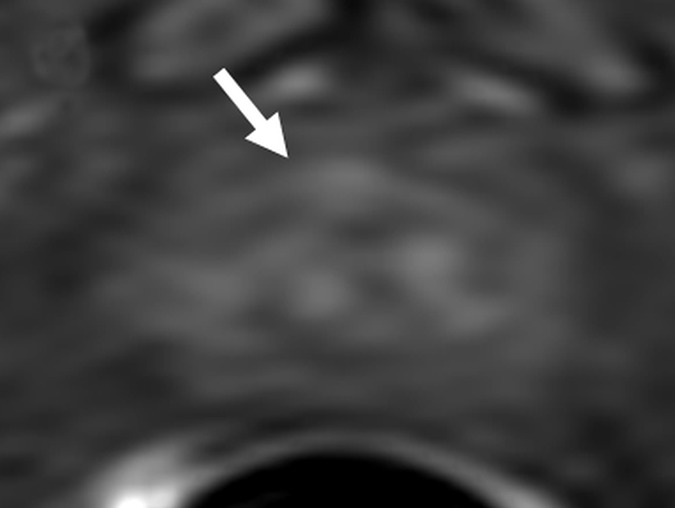
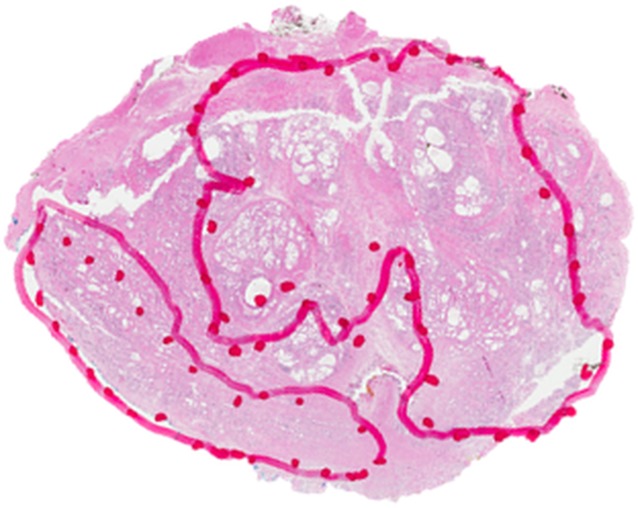
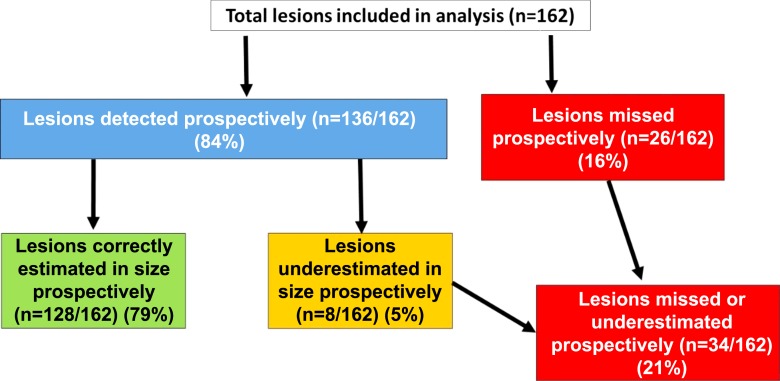
Purpose To characterize clinically important prostate cancers missed at multiparametric (MP) magnetic resonance (MR) imaging. Materials and Methods The local institutional review board approved this HIPAA-compliant retrospective single-center study, which included 100 consecutive patients who had undergone MP MR imaging and subsequent radical prostatectomy. A genitourinary pathologist blinded to MP MR findings outlined prostate cancers on whole-mount pathology slices. Two readers correlated mapped lesions with reports of prospectively read MP MR images. Readers were blinded to histopathology results during prospective reading. At histopathologic examination, 80 clinically unimportant lesions (<5 mm; Gleason score, 3+3) were excluded. The same two readers, who were not blinded to histopathologic findings, retrospectively reviewed cancers missed at MP MR imaging and assigned a Prostate Imaging Reporting and Data System (PI-RADS) version 2 score to better understand false-negative lesion characteristics. Descriptive statistics were used to define patient characteristics, including age, prostate-specific antigen (PSA) level, PSA density, race, digital rectal examination results, and biopsy results before MR imaging. Student t test was used to determine any demographic differences between patients with false-negative MP MR imaging findings and those with correct prospective identification of all lesions. Results Of the 162 lesions, 136 (84%) were correctly identified with MP MR imaging. Size of eight lesions was underestimated. Among the 26 (16%) lesions missed at MP MR imaging, Gleason score was 3+4 in 17 (65%), 4+3 in one (4%), 4+4 in seven (27%), and 4+5 in one (4%). Retrospective PI-RADS version 2 scores were assigned (PI-RADS 1, n = 8; PI-RADS 2, n = 7; PI-RADS 3, n = 6; and PI-RADS 4, n = 5). On a per-patient basis, MP MR imaging depicted clinically important prostate cancer in 99 of 100 patients. At least one clinically important tumor was missed in 26 (26%) patients, and lesion size was underestimated in eight (8%). Conclusion Clinically important lesions can be missed or their size can be underestimated at MP MR imaging. Of missed lesions, 58% were not seen or were characterized as benign findings at second-look analysis. Recognition of the limitations of MP MR imaging is important, and new approaches to reduce this false-negative rate are needed. © RSNA, 2017 Online supplemental material is available for this article.
Figures





Comment in
-
Re: What Are We Missing? False-negative Cancers at Multiparametric MR Imaging of the Prostate.Eur Urol. 2018 Apr;73(4):637. doi: 10.1016/j.eururo.2017.12.006. Epub 2017 Dec 19. Eur Urol. 2018. PMID: 29273407 No abstract available.
-
Deep Learning or Fundamental Descriptors?Radiology. 2018 May;287(2):728-729. doi: 10.1148/radiol.2017173053. Radiology. 2018. PMID: 29668415 No abstract available.
-
68Ga Prostate-specific Membrane Antigen PET/CT for Primary Diagnosis of Prostate Cancer: Complementary or Alternative to Multiparametric MR Imaging.Radiology. 2018 May;287(2):725-726. doi: 10.1148/radiol.2017172607. Radiology. 2018. PMID: 29668418 No abstract available.
References
-
- Damber JE, Aus G. Prostate cancer. Lancet 2008;371(9625):1710–1721. - PubMed
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011;61(2):69–90. - PubMed
-
- Fütterer JJ, Heijmink SW, Scheenen TW, et al. Prostate cancer localization with dynamic contrast-enhanced MR imaging and proton MR spectroscopic imaging. Radiology 2006;241(2):449–458. - PubMed
-
- Haider MA, van der Kwast TH, Tanguay J, et al. Combined T2-weighted and diffusion-weighted MRI for localization of prostate cancer. AJR Am J Roentgenol 2007;189(2):323–328. - PubMed
-
- Kitajima K, Kaji Y, Fukabori Y, Yoshida K, Suganuma N, Sugimura K. Prostate cancer detection with 3 T MRI: comparison of diffusion-weighted imaging and dynamic contrast-enhanced MRI in combination with T2-weighted imaging. J Magn Reson Imaging 2010;31(3):625–631. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
