

Movement disorders with neuronal antibodies: syndromic approach, genetic parallels and pathophysiology
- PMID: 29053777
- PMCID: PMC5888977
- DOI: 10.1093/brain/awx189
Movement disorders with neuronal antibodies: syndromic approach, genetic parallels and pathophysiology
Abstract
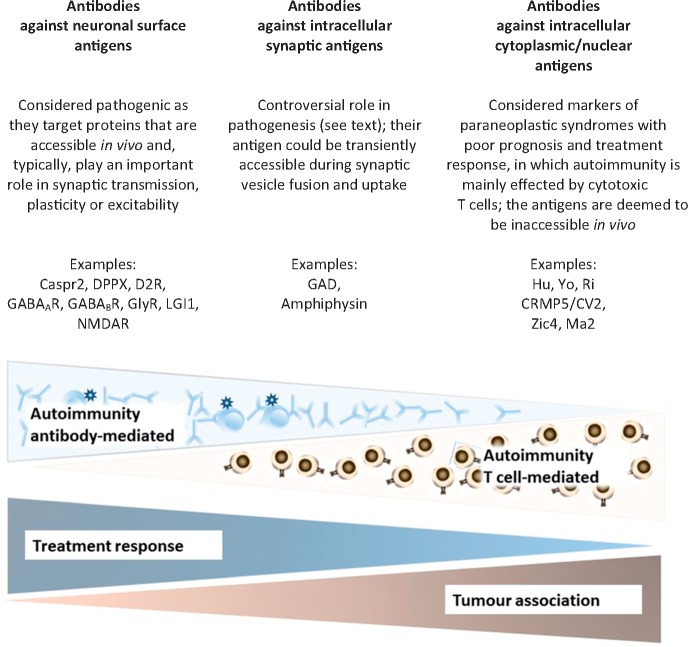
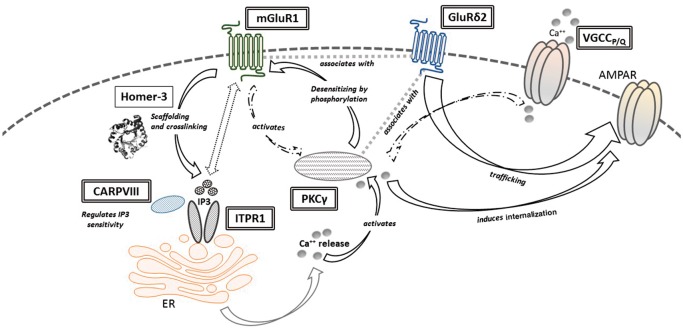
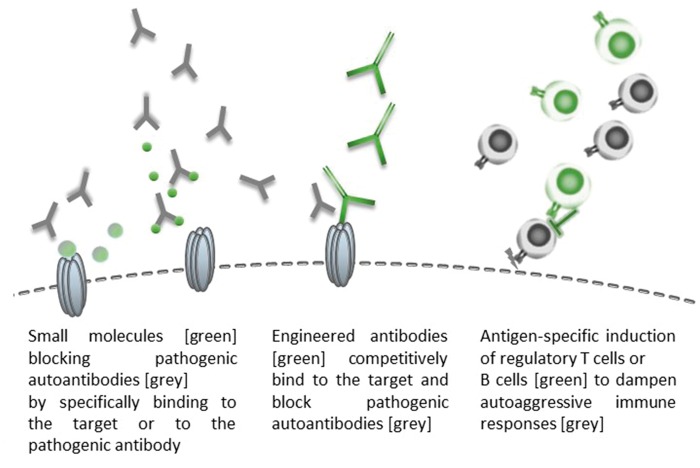
Movement disorders are a prominent and common feature in many autoantibody-associated neurological diseases, a group of potentially treatable conditions that can mimic infectious, metabolic or neurodegenerative disease. Certain movement disorders are likely to associate with certain autoantibodies; for example, the characteristic dyskinesias, chorea and dystonia associated with NMDAR antibodies, stiff person spectrum disorders with GAD, glycine receptor, amphiphysin or DPPX antibodies, specific paroxysmal dystonias with LGI1 antibodies, and cerebellar ataxia with various anti-neuronal antibodies. There are also less-recognized movement disorder presentations of antibody-related disease, and a considerable overlap between the clinical phenotypes and the associated antibody spectra. In this review, we first describe the antibodies associated with each syndrome, highlight distinctive clinical or radiological 'red flags', and suggest a syndromic approach based on the predominant movement disorder presentation, age, and associated features. We then examine the underlying immunopathophysiology, which may guide treatment decisions in these neuroimmunological disorders, and highlight the exceptional interface between neuronal antibodies and neurodegeneration, such as the tauopathy associated with IgLON5 antibodies. Moreover, we elaborate the emerging pathophysiological parallels between genetic movement disorders and immunological conditions, with proteins being either affected by mutations or targeted by autoantibodies. Hereditary hyperekplexia, for example, is caused by mutations of the alpha subunit of the glycine receptor leading to an infantile-onset disorder with exaggerated startle and stiffness, whereas antibodies targeting glycine receptors can induce acquired hyperekplexia. The spectrum of such immunological and genetic analogies also includes cerebellar ataxias and some encephalopathies. Lastly, we discuss how these pathophysiological considerations could reflect on possible future directions regarding antigen-specific immunotherapies or targeting the pathophysiological cascades downstream of the antibody effects.
Keywords: ataxia; chorea; movement disorders; neuronal antibodies; parkinsonism.
© The Author (2017). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Abgrall G, Demeret S, Rohaut B, Leu-Semenescu S, Arnulf I. Status dissociatus and disturbed dreaming in a patient with Morvan syndrome plus Myasthenia Gravis. Sleep Med 2015; 16: 894–6. - PubMed
-
- Angus-Leppan H, Rudge P, Mead S, Collinge J, Vincent A. Autoantibodies in sporadic Creutzfeldt-Jakob disease. JAMA Neurol 2013; 70: 919–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
