

Incremental Prognostic Utility of Left Ventricular Global Longitudinal Strain in Hypertrophic Obstructive Cardiomyopathy Patients and Preserved Left Ventricular Ejection Fraction
- PMID: 29054839
- PMCID: PMC5721859
- DOI: 10.1161/JAHA.117.006514
Incremental Prognostic Utility of Left Ventricular Global Longitudinal Strain in Hypertrophic Obstructive Cardiomyopathy Patients and Preserved Left Ventricular Ejection Fraction
Abstract
Background: In obstructive hypertrophic cardiomyopathy patients with preserved left ventricular (LV) ejection fraction, we sought to determine whether LV global longitudinal strain (LV-GLS) provided incremental prognostic utility.
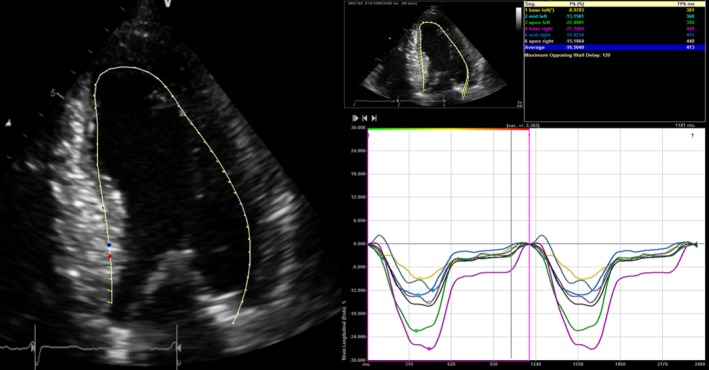
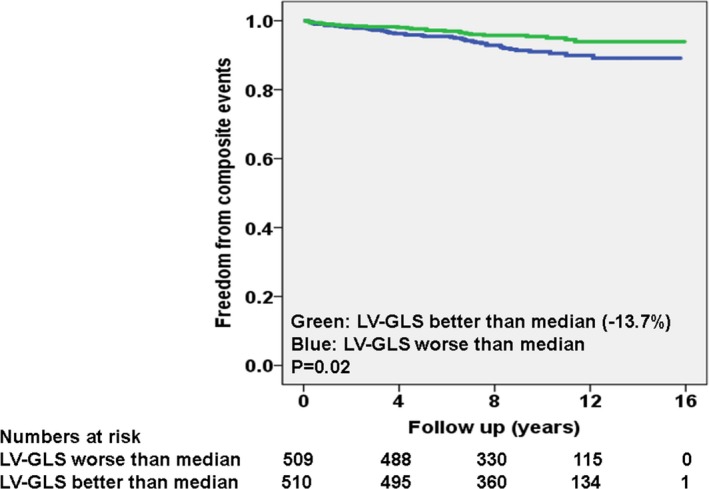
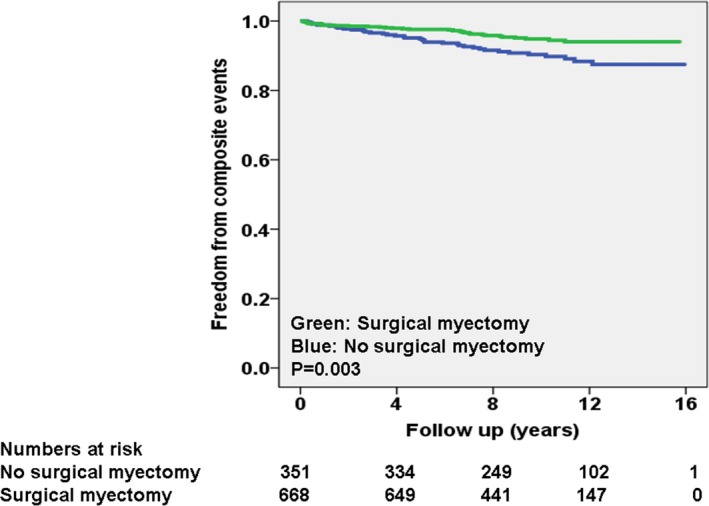
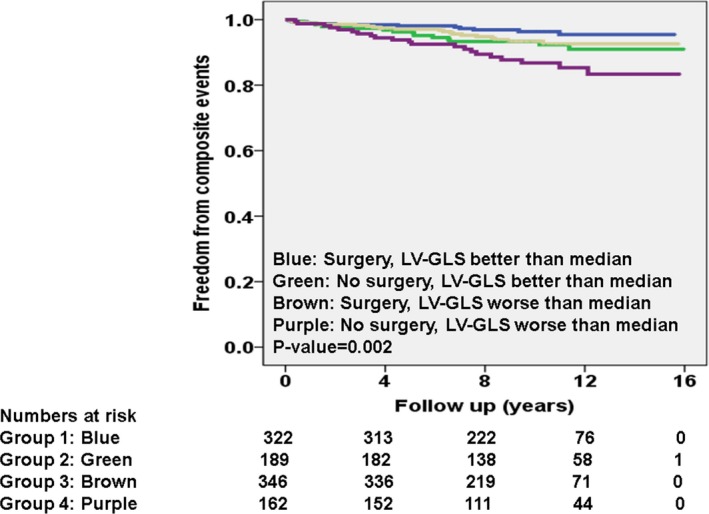
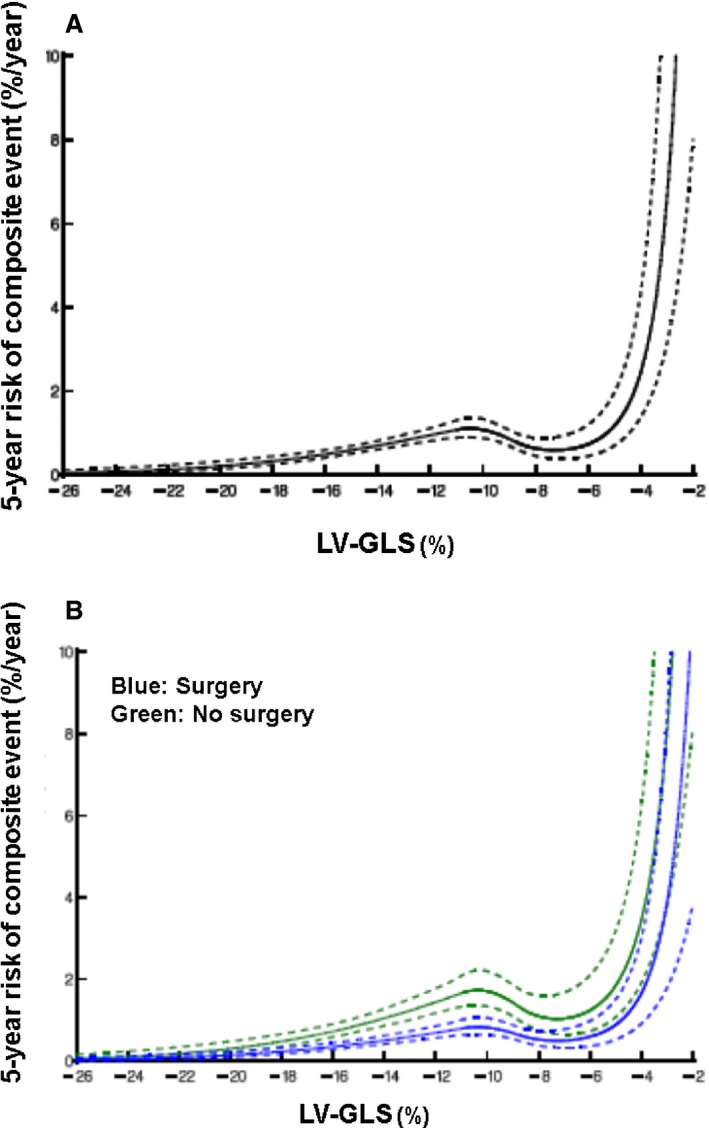
Methods and results: We studied 1019 patients with documented hypertrophic cardiomyopathy (mean age, 50±12 years; 63% men) evaluated at our center between 2001 and 2011. We excluded age <18 years, maximal LV outflow tract gradient <30 mm Hg, bundle branch block or atrial fibrillation, past pacemaker/cardiac surgery, including myectomy/alcohol ablation, and obstructive coronary artery disease. Average resting LV-GLS was measured offline on 2-, 3-, 4-chamber views using Velocity Vector Imaging (Siemens, Malvern, PA). Outcome was a composite of cardiac death and appropriate internal defibrillator (implantable cardioverter defibrillator) discharge. Maximal LV thickness, LV ejection fraction, indexed left atrial dimension, rest and maximal LV outflow tract gradient, and LV-GLS were 2.0±0.2 cm, 62±4%, 2.2±4 cm/m2, 52±42 mm Hg, 103±36 mm Hg, and -13.6±4%. During 9.4±3 years of follow-up, 668 (66%), 166 (16%), and 122 (20%), respectively, had myectomy, atrial fibrillation, and implantable cardioverter defibrillator implantation, whereas 69 (7%) had composite events (62 cardiac deaths). Multivariable competing risk regression analysis revealed that higher age (subhazard ratio, 1.04 [1.02-1.07]), AF during follow-up (subhazard ratio, 1.39 [1.11-1.69]), and worsening LV-GLS (subhazard ratio, 1.11 [1.05-1.22]) were associated with worse outcomes, whereas myectomy (subhazard ratio, 0.44 [0.25-0.72]) was associated with improved outcomes (all P<0.01). Sixty-one percent of events occurred in patients with LV-GLS worse than median (-13.7%).
Conclusions: In obstructive hypertrophic cardiomyopathy patients with preserved LV ejection fraction, abnormal LV-GLS was independently associated with higher events, whereas myectomy was associated with improved outcomes.
Keywords: hypertrophic cardiomyopathy; outcome; strain.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:e783–e831. - PubMed
-
- Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege AA, Lafont A, Limongelli G, Mahrholdt H, McKenna WJ, Mogensen J, Nihoyannopoulos P, Nistri S, Pieper PG, Pieske B, Rapezzi C, Rutten FH, Tillmanns C, Watkins H. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014;35:2733–2779. - PubMed
-
- Maron MS, Olivotto I, Betocchi S, Casey SA, Lesser JR, Losi MA, Cecchi F, Maron BJ. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003;348:295–303. - PubMed
-
- Elliott PM, Gimeno JR, Tome MT, Shah J, Ward D, Thaman R, Mogensen J, McKenna WJ. Left ventricular outflow tract obstruction and sudden death risk in patients with hypertrophic cardiomyopathy. Eur Heart J. 2006;27:1933–1941. - PubMed
-
- Maron MS, Olivotto I, Zenovich AG, Link MS, Pandian NG, Kuvin JT, Nistri S, Cecchi F, Udelson JE, Maron BJ. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation. 2006;114:2232–2239. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
