

The Pathophysiology of Dry Eye Disease: What We Know and Future Directions for Research
- PMID: 29055361
- PMCID: PMC5657523
- DOI: 10.1016/j.ophtha.2017.07.010
The Pathophysiology of Dry Eye Disease: What We Know and Future Directions for Research
Abstract
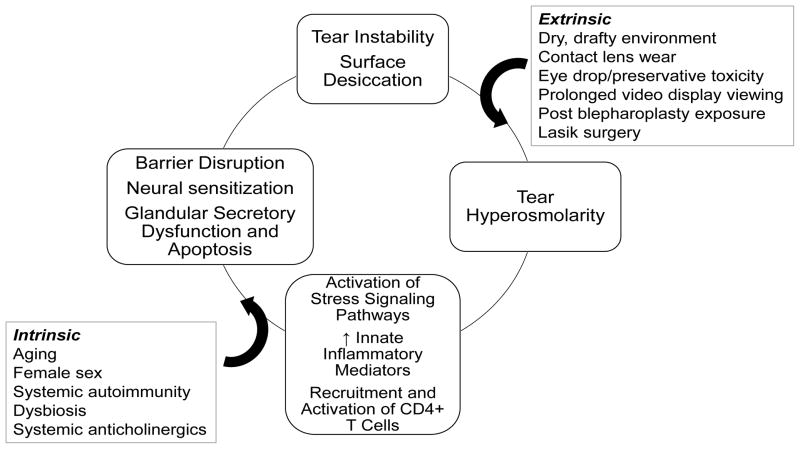
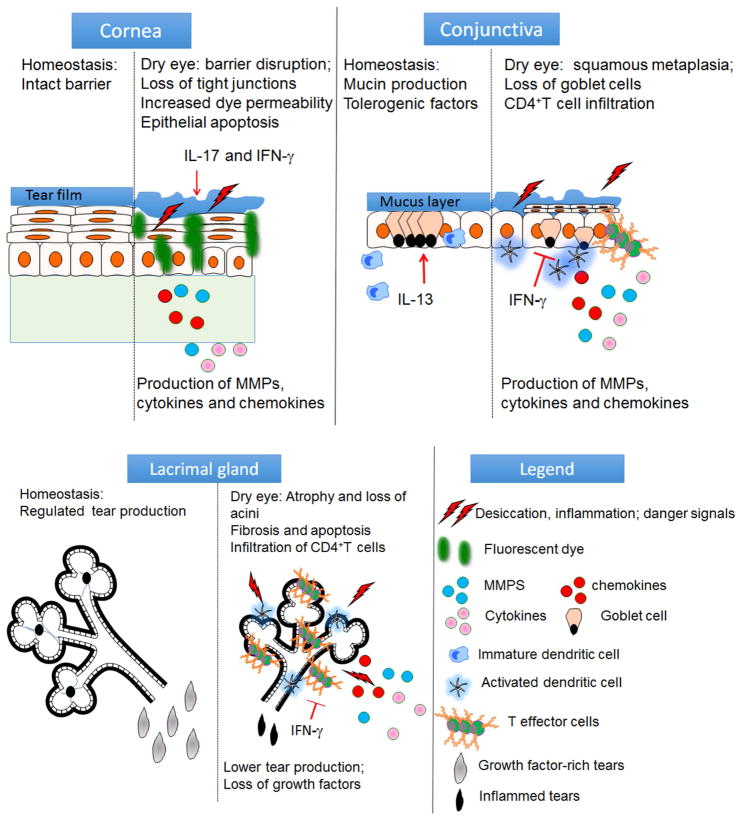
Clinical and laboratory studies performed over the past few decades have discovered that dry eye is a chronic inflammatory disease that can be initiated by numerous extrinsic or intrinsic factors that promote an unstable and hyperosmolar tear film. These changes in tear composition, in some cases combined with systemic factors, lead to an inflammatory cycle that causes ocular surface epithelial disease and neural stimulation. Acute desiccation activates stress signaling pathways in the ocular surface epithelium and resident immune cells. This triggers production of innate inflammatory mediators that stimulate the production of matrix metalloprotease, inflammatory cell recruitment, and dendritic cell maturation. These mediators, combined with exposure of autoantigens, can lead to an adaptive T cell-mediated response. Cornea barrier disruption develops by protease-mediated lysis of epithelial tight junctions, leading to accelerated cell death; desquamation; an irregular, poorly lubricated cornea surface; and exposure and sensitization of epithelial nociceptors. Conjunctival goblet cell dysfunction and death are promoted by the T helper 1 cytokine interferon gamma. These epithelial changes further destabilize the tear film, amplify inflammation, and create a vicious cycle. Cyclosporine and lifitegrast, the 2 US Food and Drug Administration-approved therapies, inhibit T-cell activation and cytokine production. Although these therapies represent a major advance in dry eye therapy, they are not effective in improving discomfort and corneal epithelial disease in all patients. Preclinical studies have identified other potential therapeutic targets, biomarkers, and strategies to bolster endogenous immunoregulatory pathways. These discoveries will, it is hoped, lead to further advances in diagnostic classification and treatment.
Copyright © 2017 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007) Ocul Surf. 2007;5(2):75–92. listed na. - PubMed
-
- Pflugfelder SC, de Paiva CS, Villarreal AL, Stern ME. Effects of sequential artificial tear and cyclosporine emulsion therapy on conjunctival goblet cell density and transforming growth factor-beta2 production. Cornea. 2008;27(1):64–9. - PubMed
-
- Pflugfelder SC, Stern ME. Mucosal environmental sensors in the pathogenesis of dry eye. Expert Rev Clin Immunol. 2014;10(9):1137–40. - PubMed
-
- Stern ME, Gao J, Schwalb TA, et al. Conjunctival T-cell subpopulations in Sjogren’s and non-Sjogren’s patients with dry eye. Invest Ophthalmol Vis Sci. 2002;43(8):2609–14. - PubMed
-
- Hingorani M, Metz D, Lightman SL. Characterisation of the normal conjunctival leukocyte population. Exp Eye Res. 1997;64(6):905–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
