

LGI1, CASPR2 and related antibodies: a molecular evolution of the phenotypes
- PMID: 29055902
- PMCID: PMC5909759
- DOI: 10.1136/jnnp-2017-315720
LGI1, CASPR2 and related antibodies: a molecular evolution of the phenotypes
Abstract
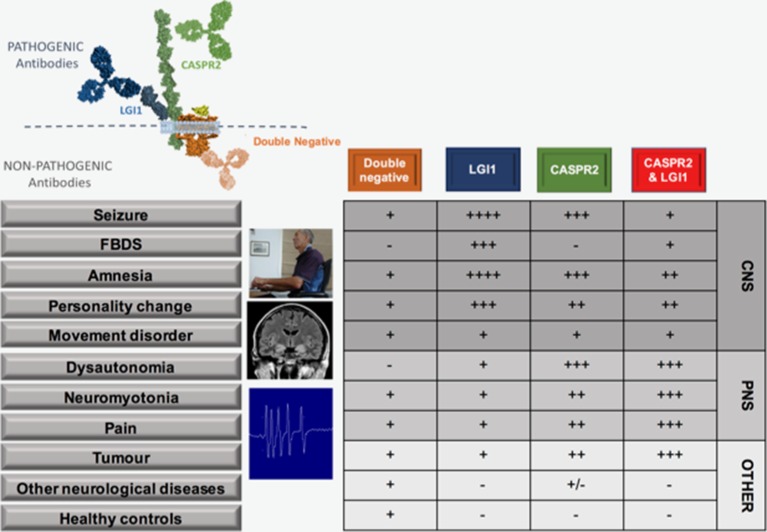
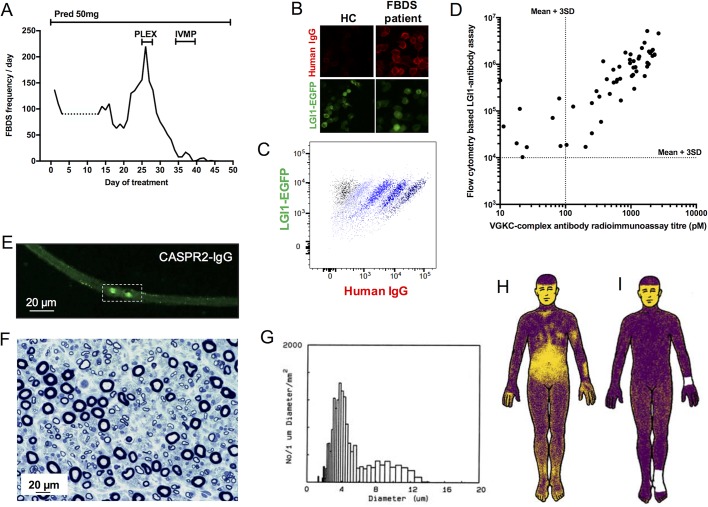
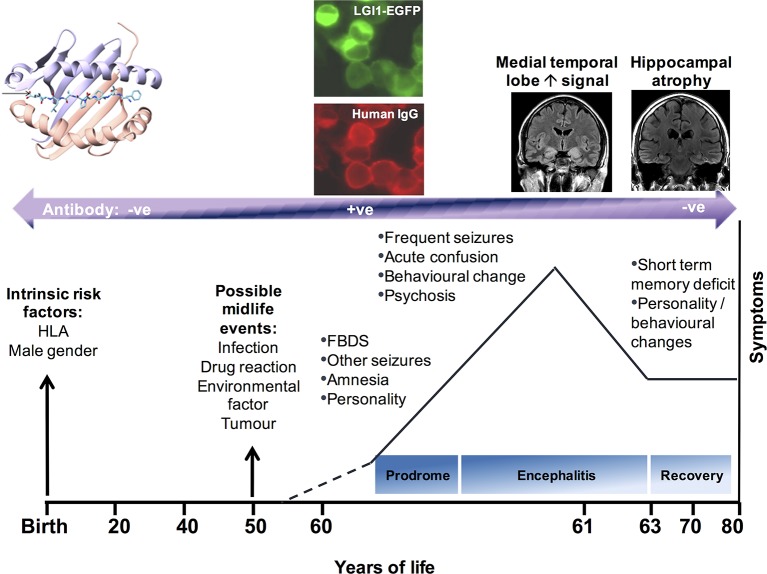
Recent biochemical observations have helped redefine antigenic components within the voltage-gated potassium channel (VGKC) complex. The related autoantibodies may be now divided into likely pathogenic entities, which target the extracellular domains of leucine-rich glioma-inactivated 1 (LGI1) and contactin-associated protein-like 2 (CASPR2), and species that target intracellular neuronal components and are likely non-pathogenic. This distinction has enhanced clinical practice as direct determination of LGI1 and CASPR2 antibodies offers optimal sensitivity and specificity. In this review, we describe and compare the clinical features associated with pathogenic LGI1 and CASPR2 antibodies, illustrate emerging laboratory techniques for antibody determination and describe the immunological mechanisms that may mediate antibody-induced pathology. We highlight marked clinical overlaps between patients with either LGI1 or CASPR2 antibodies that include frequent focal seizures, prominent amnesia, dysautonomia, neuromyotonia and neuropathic pain. Although occurring at differing rates, these commonalities are striking and only faciobrachial dystonic seizures reliably differentiate these two conditions. Furthermore, the coexistence of both LGI1 and CASPR2 antibodies in an individual occurs surprisingly frequently. Patients with either antibody respond well to immunotherapies, although systematic studies are required to determine the magnitude of the effect beyond placebo. Finally, data have suggested that CASPR2 and LGI1 modulation via genetic or autoimmune mechanisms may share common intermediate molecules. Taken together, the biochemical distinction of antigenic targets has led to important clinical advances for patient care. However, the striking syndrome similarities, coexistence of two otherwise rare antibodies and molecular insights suggest the VGKC complex may yet be a common functional effector of antibody action. Hence, we argue for a molecular evolution alongside a clinical and phenotypic re-evaluation.
Keywords: autoimmune encephalitis; epilepsy; limbic system; neuroimmunology; paraneoplastic syndrome.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: SRI and PW are coapplicants and receive royalties on patent application WO/2010/046716 (UK patent no.: PCT/GB2009/051441) entitled ’Neurological Autoimmune Disorders'. The patent has been licenced to Euroimmun AG for the development of assays for LGI1 and other VGKC complex antibodies.
Figures
References
-
- Irani SR, Alexander S, Waters P, et al. Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan’s syndrome and acquired neuromyotonia. Brain 2010;133:2734–48. 10.1093/brain/awq213 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources