

Development of a Patient-specific Tumor Mold Using Magnetic Resonance Imaging and 3-Dimensional Printing Technology for Targeted Tissue Procurement and Radiomics Analysis of Renal Masses
- PMID: 29056576
- PMCID: PMC5885749
- DOI: 10.1016/j.urology.2017.08.056
Development of a Patient-specific Tumor Mold Using Magnetic Resonance Imaging and 3-Dimensional Printing Technology for Targeted Tissue Procurement and Radiomics Analysis of Renal Masses
Abstract
Objective: To implement a platform for colocalization of in vivo quantitative multiparametric magnetic resonance imaging features with ex vivo surgical specimens of patients with renal masses using patient-specific 3-dimensional (3D)-printed tumor molds, which may aid in targeted tissue procurement and radiomics and radiogenomic analyses.
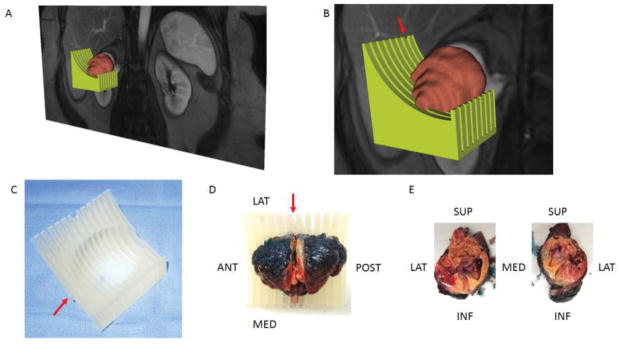
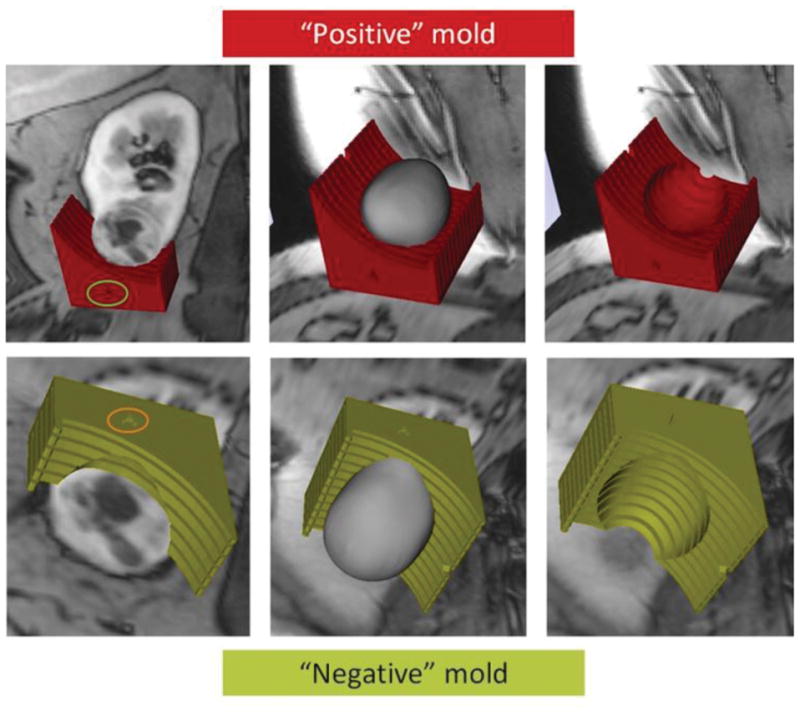
Materials and methods: Volumetric segmentation of 6 renal masses was performed with 3D Slicer (http://www.slicer.org) to create a 3D tumor model. A slicing guide template was created with specialized software, which included notches corresponding to the anatomic locations of the magnetic resonance images. The tumor model was subtracted from the slicing guide to create a depression in the slicing guide corresponding to the exact size and shape of the tumor. A customized, tumor-specific, slicing guide was then printed using a 3D printer. After partial nephrectomy, the surgical specimen was bivalved through the preselected magnetic resonance imaging (MRI) plane. A thick slab of the tumor was obtained, fixed, and processed as a whole-mount slide and was correlated to multiparametric MRI findings.
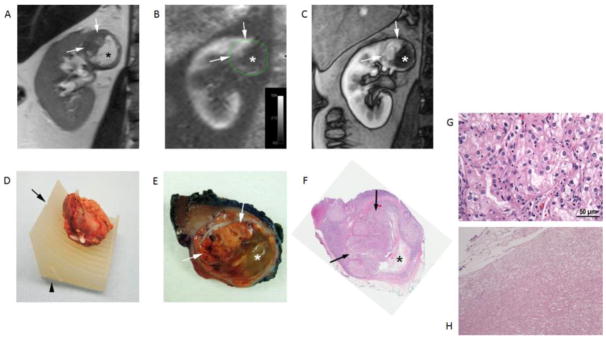
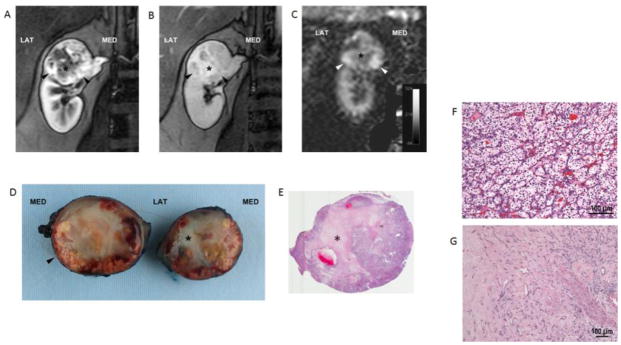
Results: All patients successfully underwent partial nephrectomy and adequate fitting of the tumor specimens within the 3D mold was achieved in all tumors. Distinct in vivo MRI features corresponded to unique pathologic characteristics in the same tumor. The average cost of printing each mold was US$160.7 ± 111.1 (range: US$20.9-$350.7).
Conclusion: MRI-based preoperative 3D printing of tumor-specific molds allow for accurate sectioning of the tumor after surgical resection and colocalization of in vivo imaging features with tissue-based analysis in radiomics and radiogenomic studies.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Segal E, Sirlin CB, Ooi C, et al. Decoding global gene expression programs in liver cancer by noninvasive imaging. Nat Biotechnol. 2007;25:675–680. - PubMed
-
- Jamshidi N, Jonasch E, Zapala M, et al. The Radiogenomic Risk Score: Construction of a Prognostic Quantitative, Noninvasive Image-based Molecular Assay for Renal Cell Carcinoma. Radiology. 2015;277:114–123. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
