

Lymphatic pathology in asymptomatic and symptomatic children with Wuchereria bancrofti infection in children from Odisha, India and its reversal with DEC and albendazole treatment
- PMID: 29059186
- PMCID: PMC5667936
- DOI: 10.1371/journal.pntd.0005631
Lymphatic pathology in asymptomatic and symptomatic children with Wuchereria bancrofti infection in children from Odisha, India and its reversal with DEC and albendazole treatment
Abstract
Background: Once interruption of transmission of lymphatic filariasis is achieved, morbidity prevention and management becomes more important. A study in Brugia malayi filariasis from India has shown sub-clinical lymphatic pathology with potential reversibility. We studied a Wuchereria bancrofti infected population, the major contributor to LF globally.
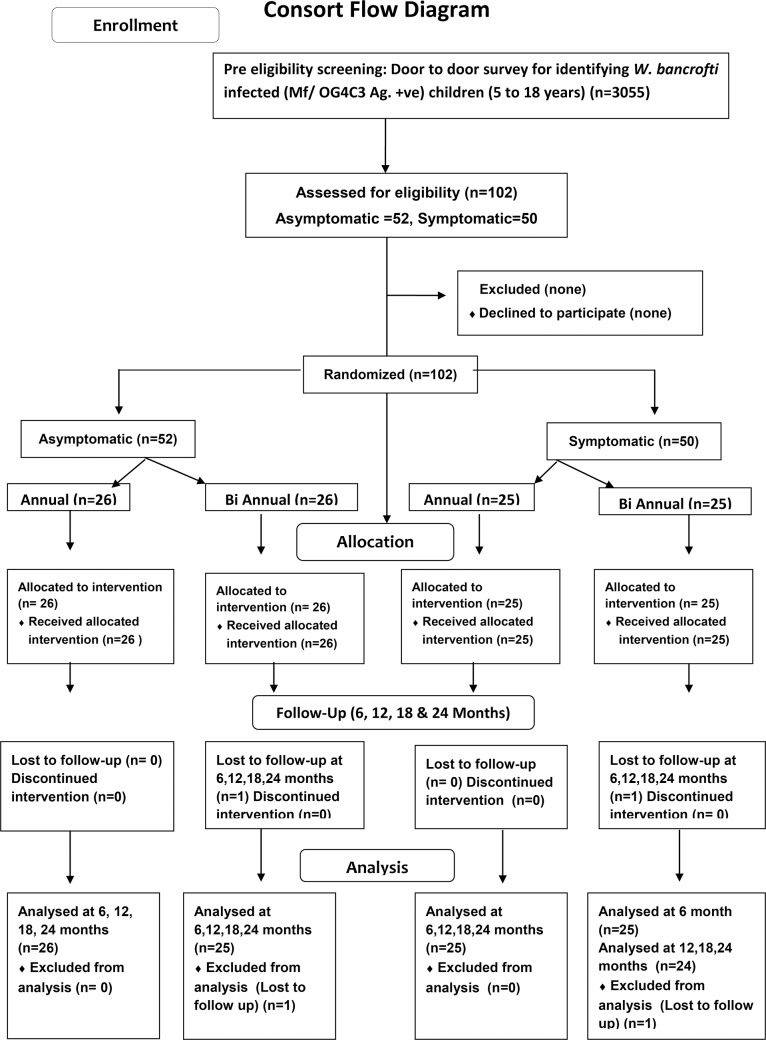
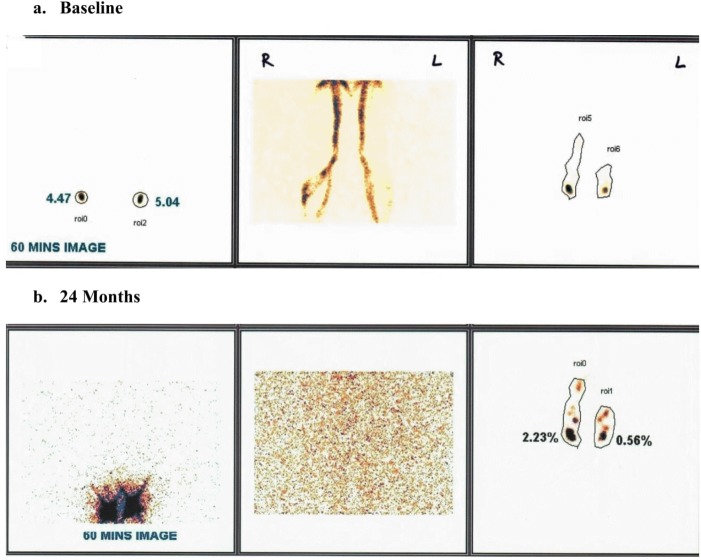
Methods: Children aged 5-18 years from Odisha, India were screened for W. bancrofti infection and disease. 102 infected children, 50 with filarial disease and 52 without symptoms were investigated by lymphoscintigraphy and then randomized to receive a supervised single oral dose of DEC and albendazole which was repeated either annually or semi-annually. The lymphatic pathology was evaluated six monthly for two years.
Findings: Baseline lymphoscintigraphy showed abnormality in lower limb lymphatics in 80% of symptomatic (40/50) and 63·5% (33/52) of asymptomatic children. Progressive improvement in baseline pathology was seen in 70·8, 87·3, 98·6, and 98·6% of cases at 6, 12, 18, and 24 months follow up, while in 4·2, 22·5, 47·9 and 64·8%, pathology reverted to normal. This was independent of age (p = 0·27), symptomatic status (p = 0·57) and semi-annual/bi-annual dosing (p = 0·46). Six of eleven cases showed clinical reduction in lymphedema of legs.
Interpretation: A significant proportion of a young W. bancrofti infected population exhibited lymphatic pathology which was reversible with annual dosage of DEC and albendazole. This provides evidence for morbidity prevention & treatment of early lymphedema. It can also be used as a tool to improve community compliance during mass drug administration.
Trial registration: ClinicalTrials.gov No CTRI/2013/10/004121.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures








References
-
- de Kraker ME, Stolk WA, van Oortmarssen GJ, Habbema JD. Model-based analysis of trial data: microfilaria and worm productivity loss after diethylcarbamazine-albendazole or ivermectin-albendazole combination therapy against Wuchereria bancrofti. Trop Med Int Health. 2006; 11: 718–728. doi: 10.1111/j.1365-3156.2006.01606.x - DOI - PubMed
-
- Ramaiah KD, Vijay Kumar KN, Ravi R, Das PK. Situation analysis in a large urban area of India, prior to launching a programme of mass drug administrations to eliminate lymphatic filariasis. Ann Trop Med Parasitol. 2005; 99: 243–252. doi: 10.1179/136485905X29701 - DOI - PubMed
-
- Addiss DG, Louis-Charles J, Roberts J, Leconte F, Wendt JM, Milord MD, et al. Feasibility and effectiveness of basic lymphedema management in Leogane, Haiti, an area endemic for bancroftian filariasis. PLoS Negl Trop Dis. 2010; 4: e668 doi: 10.1371/journal.pntd.0000668 - DOI - PMC - PubMed
-
- Kerketta AS, Babu BV, Rath K, Jangid PK, Nayak AN, Kar SK. A randomized clinical trial to compare the efficacy of three treatment regimens along with foot care in the morbidity management of filarial lymphedema. Trop Med Int Health. 2005; 10: 698–705. doi: 10.1111/j.1365-3156.2005.01442.x - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
