

High-frequency burst vagal nerve simulation therapy in a natural primate model of genetic generalized epilepsy
- PMID: 29059589
- PMCID: PMC5856459
- DOI: 10.1016/j.eplepsyres.2017.10.010
High-frequency burst vagal nerve simulation therapy in a natural primate model of genetic generalized epilepsy
Abstract
Purpose: Since the approval of Vagal Nerve Stimulation (VNS) Therapy for medically refractory focal epilepsies in 1997, it has been also reported to be effective for a wide range of generalized seizures types and epilepsy syndromes. Instead of conventional VNS Therapy delivered at 20-30Hz signal frequencies, this study evaluates efficacy and tolerability of high-frequency burst VNS in a natural animal model for genetic generalized epilepsy (GGE), the epileptic baboon.
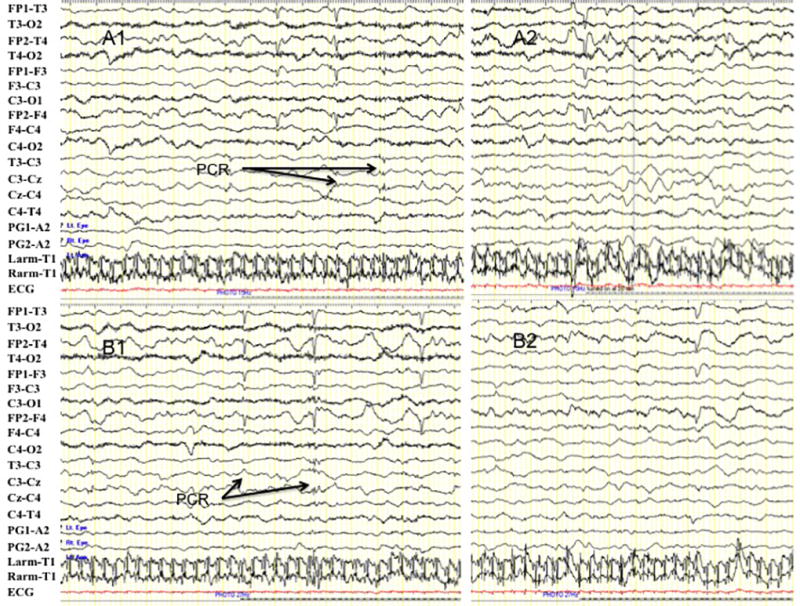
Methods: Two female baboons (B1 P.h. Hamadryas and B2 P.h. Anubis x Cynocephalus) were selected because of frequently witnessed generalized tonic-clonic seizures (GTCS) for VNS implantation. High-frequency burst VNS Therapy was initiated after a 4-5 week baseline; different VNS settings (0.25, 2 or 2.5mA, 300Hz, 4 vs 7 pulses, 0.5-2.5s interburst interval, and intermittent stimulation for 1-2 vs for 24h per day) were tested over the subsequent 19 weeks, which included a 4-6 week wash-out period. GTCS frequencies were quantified for each setting, while seizure duration and postictal recovery times were compared to baseline. Scalp EEG studies were performed at almost every setting, including intermittent light stimulation (ILS) to evaluate photosensitivity. Pre-ILS ictal and interictal discharge rates, as well as ILS responses were compared between trials. The Novel Object test was used to assess potential treatment effects on behavior.
Results: High-frequency burst VNS Therapy reduced GTCS frequencies at all treatment settings in both baboons, except when output currents were reduced (0.25mA) or intermittent stimulation was restricted (to 1-2h/day). Seizure duration and postictal recovery times were unchanged. Scalp EEG studies did not demonstrate treatment-related decrease of ictal or interictal epileptic discharges or photosensitivity, but continuous treatment for 120-180s during ILS appeared to reduce photoparoxysmal responses. High-frequency burst VNS Therapy was well-tolerated by both baboons, without cardiac or behavioral changes. Repetitive muscle contractions involving the neck and left shoulder girdle were observed intermittently, most commonly at 0.5 interburst intervals, but these were transient, resolving with a few cycles of stimulation and not noted in wakefulness.
Conclusions: This preclinical pilot study demonstrates efficacy and tolerability of high-frequency burst VNS Therapy in the baboon model of GGE. The muscle contractions may be due to aberrant propagation of the stimulus along the vagal nerve or to the ansa cervicalis, but can be reduced by minimal adjustment of current output or stimulus duration.
Keywords: Baboon; Generalized tonic-clonic seizures; High-frequency burst VNS therapy; Idiopathic generalized epilepsy; Outcome.
Copyright © 2017 Elsevier B.V. All rights reserved.
Figures

References
-
- Ben-Menachem E. Vagus nerve stimulation, side effects, and long-term safety. J. Clin. Neurophysiol. 2001;18:415–418. - PubMed
-
- Morris GL, III, Mueller WM. Long-term treatment with vagus nerve stimulation in patients with refractory epilepsy. The Vagus Nerve Stimulation Study Group E01-E05. Neurology. 1999;53:1731–1735. - PubMed
-
- Boon P, Vonck K, van Rijckevorsel K, El Tahry R, Elger CE, Mullatti N, Schulze-Bonhage A, Wagner L, Diehl B, Hamer H, Reuber M, Kostov H, Lefros B, Noachtar S, Weber YG, Coenen VA, Rooijakkar H, Schijns OC, Selmoy R, Van Roost D, Eggleston KS, Van Grunderbeek W, Jayewardene AK, McGuire RM. A prospective, multicenter study of cardiac-based seizure detection to activate vagus nerve stimulation. Seizure. 2015;32:52–61. - PubMed
-
- Handforth A, DeGiorgio CM, Schachter SC, Uthman BM, Naritoku DK, Tecoma ES, Henry TR, Collins SD, Vaughn BV, Gilmartin RC, Labar DR, Morris GL, III, Salinsky MC, Osorio I, Ristmoric RK, Labiner DM, Jones JC, Murphy JV, Ney GL, Wheless JW. Vagus nerve stimulation therapy for partial-onset seizures: a randomized active-control trial. Neurology. 1998;51:48–55. - PubMed
-
- Alexander GM, McNamara JO. Vagus nerve stimulation elevates seizure threshold in the kindling model. Epilepsia. 2012;53:2043–2052. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
