

Hepatic artery infusion chemotherapy using mFOLFOX versus transarterial chemoembolization for massive unresectable hepatocellular carcinoma: a prospective non-randomized study
- PMID: 29061175
- PMCID: PMC5654007
- DOI: 10.1186/s40880-017-0251-2
Hepatic artery infusion chemotherapy using mFOLFOX versus transarterial chemoembolization for massive unresectable hepatocellular carcinoma: a prospective non-randomized study
Abstract
Background: Transarterial chemoembolization (TACE) is recommended as the standard care for unresectable hepatocellular carcinoma (HCC) at Barcelona Clinic Liver Cancer (BCLC) stage A-B. However, the efficacy of TACE on large (≥ 10 cm) stage A-B HCC is far from satisfactory, and it is proposed that hepatic artery infusion chemotherapy (HAIC) might be a better first-line treatment of this disease. Hence, we compared the safety and efficacy of HAIC with the modified FOLFOX (mFOLFOX) regimen and those of TACE in patients with massive unresectable HCC.
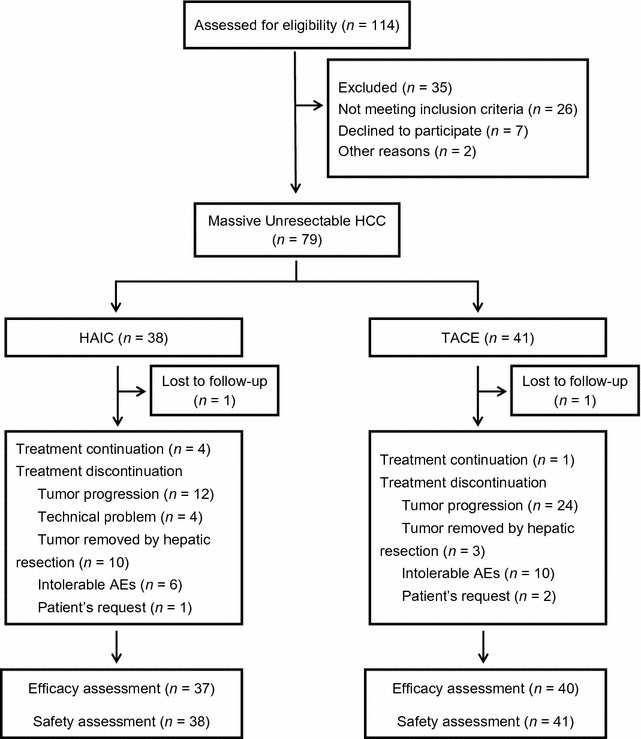
Methods: A prospective, non-randomized, phase II study was conducted on patients with massive unresectable HCC. The protocol involved HAIC with the mFOLFOX regimen (oxaliplatin, 85 mg/m2 intra-arterial infusion; leucovorin, 400 mg/m2 intra-arterial infusion; and fluorouracil, 400 mg/m2 bolus infusion and 2400 mg/m2 continuous infusion) every 3 weeks and TACE with 50 mg of epirubicin, 50 mg of lobaplatin, 6 mg of mitomycin, and lipiodol and polyvinyl alcohol particles. The tumor responses, time-to-progression (TTP), and safety were assessed.
Results: A total of 79 patients were recruited for this study: 38 in the HAIC group and 41 in the TACE group. The HAIC group exhibited higher partial response and disease control rates than did the TACE group (52.6% vs. 9.8%, P < 0.001; 83.8% vs. 52.5%, P = 0.004). The median TTPs for the HAIC and TACE groups were 5.87 and 3.6 months (hazard radio [HR] = 2.35, 95% confidence interval [CI] = 1.16-4.76, P = 0.015). More patients in the HAIC group than in the TACE group underwent resection (10 vs. 3, P = 0.033). The proportions of grade 3-4 adverse events (AE) and serious adverse events (SAE) were lower in the HAIC group than in the TACE group (grade 3-4 AEs: 13 vs. 27, P = 0.007; SAEs: 6 vs. 15, P = 0.044). More patients in the TACE group than in the HAIC group had the study treatment terminated early due to intolerable treatment-related adverse events or the withdrawal of consent (10 vs. 2, P = 0.026).
Conclusions: HAIC with mFOLFOX yielded significantly better treatment responses and less serious toxicity than did TACE. HAIC might represent a feasible and promising first-line treatment for patients with massive unresectable HCC.
Keywords: Hepatic artery infusion chemotherapy; Hepatocellular carcinoma; Transarterial chemoembolization; mFOLFOX.
Figures

References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
