

High-dose versus low-dose haemofiltration for the treatment of critically ill patients with acute kidney injury: an updated systematic review and meta-analysis
- PMID: 29061597
- PMCID: PMC5665234
- DOI: 10.1136/bmjopen-2016-014171
High-dose versus low-dose haemofiltration for the treatment of critically ill patients with acute kidney injury: an updated systematic review and meta-analysis
Abstract
Objective: The purpose of this study was to perform a systematic review and meta-analysis to evaluate the effect of high-dose versus low-dose haemofiltration on the survival of critically ill patients with acute kidney injury (AKI). We hypothesised that high-dose treatments are not associated with a higher risk of mortality.
Design: Meta-analysis.
Setting: Randomised controlled trials and two-arm prospective and retrospective studies were included.
Participants: Critically ill patients with AKI.
Interventions: Continuous renal replacement therapy.
Primary and secondary outcome measures: Primary outcomes: 90-day mortality, intensive care unit (ICU) mortality, hospital mortality; secondary outcomes: length of ICU and hospital stay.
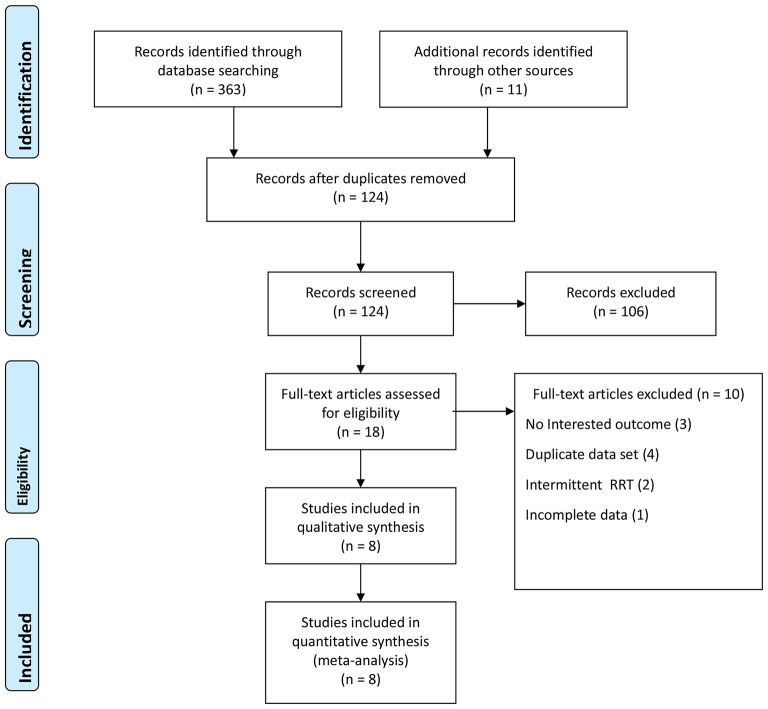
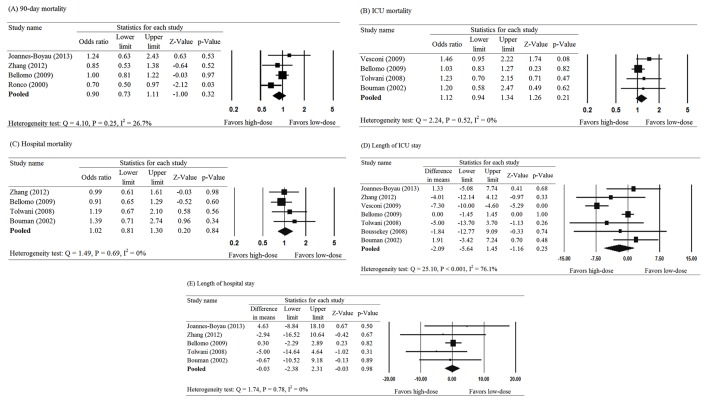
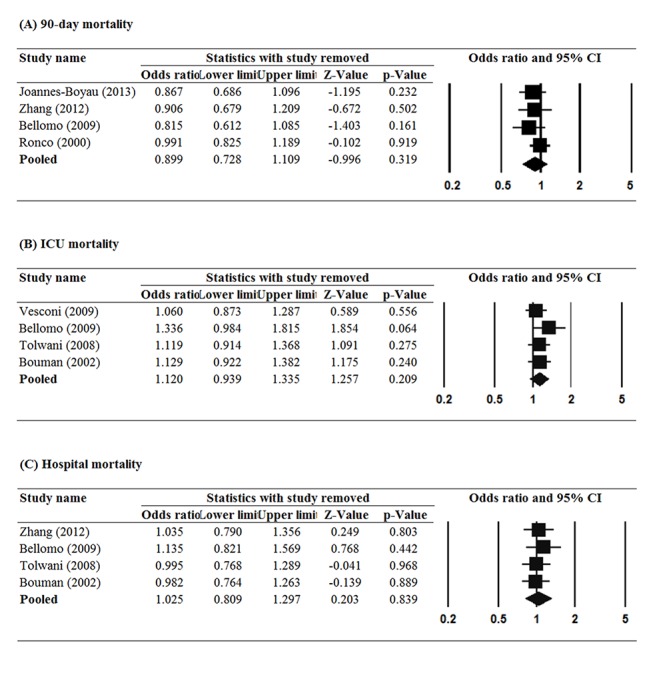
Result: Eight studies including 2970 patients were included in the analysis. Pooled results showed no significant difference in the 90-mortality rate between patients treated with high-dose or low-dose haemofiltration (pooled OR=0.90, 95% CI 0.73 to 1.11, p=0.32). Findings were similar for ICU (pooled OR=1.12, 95% CI 0.94 to 1.34, p=0.21) and hospital mortality (pooled OR=1.03, 95% CI 0.81 to 1.30, p=0.84). Length of ICU and hospital stay were similar between high-dose and low-dose groups. Pooled results are not overly influenced by any one study, different cut-off points of prescribed dose or different cut-off points of delivered dose. Meta-regression analysis indicated that the results were not affected by the percentage of patients with sepsis or septic shock.
Conclusion: High-dose and low-dose haemofiltration produce similar outcomes with respect to mortality and length of ICU and hospital stay in critically ill patients with AKI.This study was not registered at the time the data were collected and analysed. It has since been registered on 17 February 2017 at http://www.researchregistry.com/, registration number: reviewregistry211.
Keywords: acute kidney injury; dose; intensity; intensive care unit; renal dialysis; renal-replacement therapy.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources