

Bone Marrow Mononuclear Cells Combined with Beta-Tricalcium Phosphate Granules for Alveolar Cleft Repair: A 12-Month Clinical Study
- PMID: 29062005
- PMCID: PMC5653813
- DOI: 10.1038/s41598-017-12602-1
Bone Marrow Mononuclear Cells Combined with Beta-Tricalcium Phosphate Granules for Alveolar Cleft Repair: A 12-Month Clinical Study
Abstract
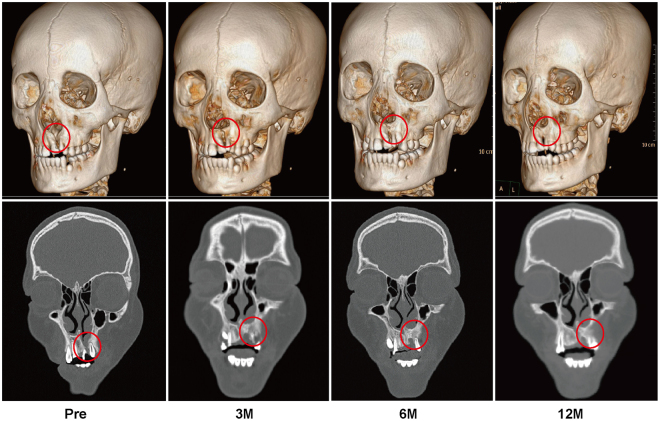
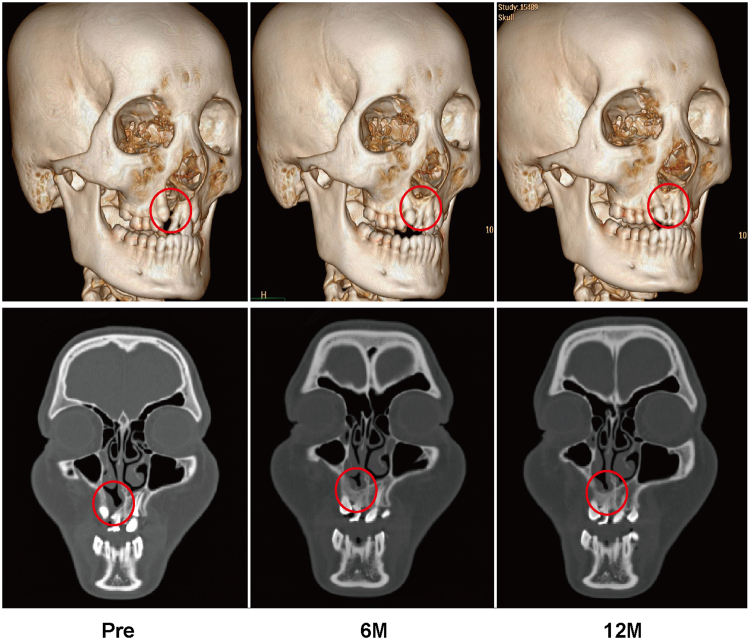
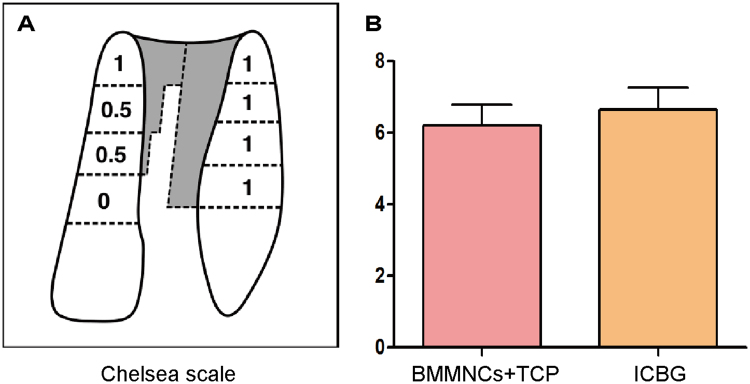
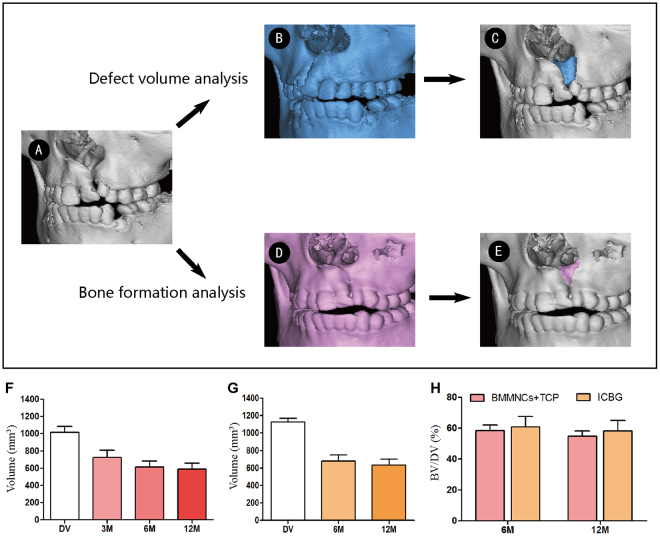
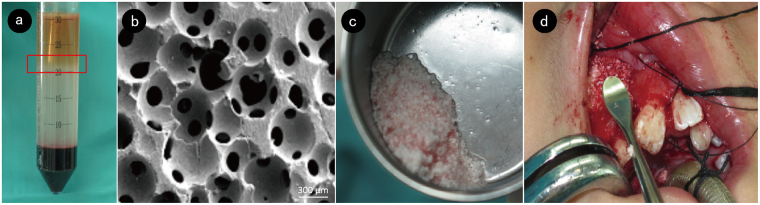
Alveolar cleft is the most common congenital bone defect. Autologous iliac crest bone graft (ICBG) is the most widely adopted procedure for alveolar cleft repair, but the condition is associated with door-site morbidities. For the first time, this study used bone marrow mononuclear cells (BMMNCs) combined with beta-tricalcium phosphate (β-TCP) granules to repair alveolar bone defect. The effectiveness of this technique was compared with autologous ICBG after 12 months of follow-up. The bone formation volume was quantitatively evaluated by three-dimensional computed tomography and computer aided engineering technology. BMMNCs/β-TCP granule grafting was radiographically equivalent to ICBG in alveolar cleft repair. Although considerable resorption was observed up to 6 months after surgery, no significant differences were noted in the Chelsea score and bone formation volume between groups. These finding indicate that BMMNCs/β-TCP grafting is a safe and effective approach for alveolar bone regeneration.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Boyne PJ, Sands NR. Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg. 1972;30:87–92. - PubMed
-
- Koole R. Ectomesenchymal mandibular symphysis bone graft: an improvement in alveolar cleft grafting? The Cleft palate-craniofacial journal: official publication of the American Cleft Palate-Craniofacial Association. 1994;31:217–223. doi: 10.1597/1545-1569(1994)031<0217:EMSBGA>2.3.CO;2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
