

Analysis of the variables affecting outcome in fractures of the tibial pilon treated by open reduction and internal fixation
- PMID: 29062214
- PMCID: PMC5647682
- DOI: 10.1016/j.jcot.2017.05.014
Analysis of the variables affecting outcome in fractures of the tibial pilon treated by open reduction and internal fixation
Abstract
Objective: To assess variables that could be related to outcomes in fractures of the tibial pilon treated by open reduction and internal fixation (ORIF).
Design: Retrospective.
Setting: University Hospital.
Patients: A total 92 fractures of the tibial pilon treated by ORIF in a 5-year period. The minimum follow-up was 1 year (mean: 3.3 years; range: 1-5).
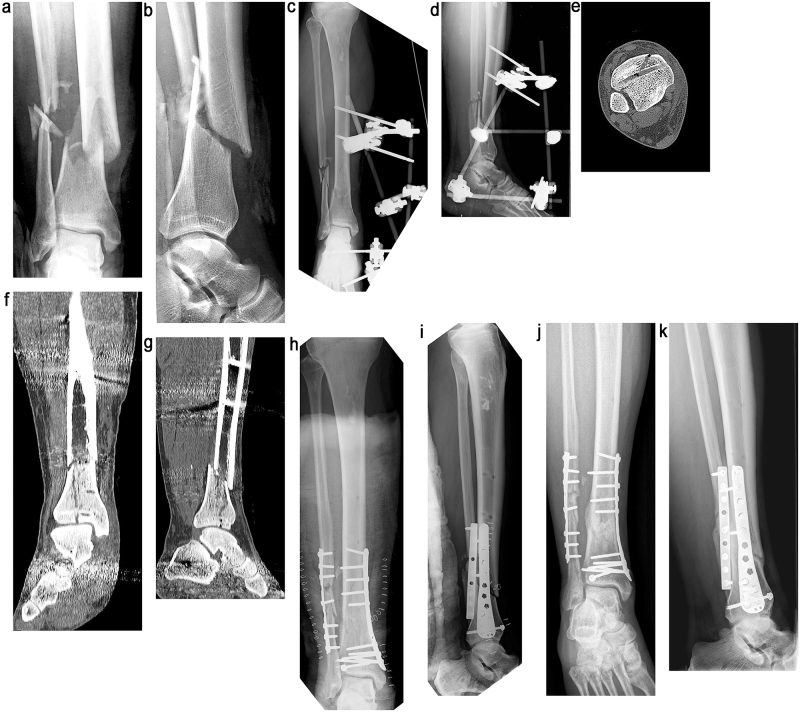
Intervention: ORIF with LCP-LISS plate.
Primary outcome measurements: Age, sex, side, type of fracture, energy of the injury, provisional external fixation (EF), time until ORIF, stages of treatment (one or two), surgical approach, type of bone fixation, quality of reduction, bone graft, hardware removal, associated fractures (fibula and others), functional results (AOFAS scale), rates of infection, skin necrosis, flap coverage, non-union, and early posttraumatic ankle osteoarthritis (AOA).
Results: According to AOFAS scale 30.5% of results were excellent, 46.7% good, 13.1% fair and 9.7% poor. Overall, the rate of infection was 13.04%, The rate of non-union was 10.86%. The rate of skin necrosis was 7.6% and the rate of flap coverage was 13.04%. The rate of early posttraumatic AOA was 13.04%. Type 43C3 fractures of the AO classification had a higher rate of skin necrosis and flap coverage. Open fractures were related to a higher prevalence of nonunion and flap coverage. The use of a bone graft was associated with a higher rate of nonunion and poor results. Infection was related to a higher prevalence of fair and poor results. EF was associated with a higher need for flap coverage. A suboptimal anatomic reduction was related to a higher rate of fair and poor results. The anteromedial approach was associated with a higher prevalence of skin necrosis and early posttraumatic AOA than the anterolateral approach. The use of an medial plate was related to a higher rate of nonunion than the use of a lateral plate.
Conclusions: The anteromedial approach was associated with a higher rate of skin necrosis and posttraumatic AOA than the anterolateral approach. Medial plating had a higher prevalence of nonunion than lateral plating.
Level of evidence: IV (case series).
Keywords: Complications; Fractures; Osteosynthesis; Outcomes; Tibial pilon.
Figures

Comment in
-
Die Pilon-tibiale-Fraktur – welche Parameter beeinflussen das Outcome in der operativen Versorgung?Z Orthop Unfall. 2018 Feb;156(1):16-17. doi: 10.1055/s-0043-122437. Epub 2018 Feb 15. Z Orthop Unfall. 2018. PMID: 29448277 German. No abstract available.
References
-
- Korkmaz A., Ciftdemir M., Ozcan M., Copuroğlu C., Sarıdoğan K. The analysis of the variables, affecting outcome in surgically treated tibia pilon fractured patients. Injury. 2013;44:1270–1274. - PubMed
-
- Bonar S.K., Marsh J.L. Tibial plafond fractures: changing principles of treatment. J Am Acad Orthop Surg. 1994;2:297–305. - PubMed
-
- Trumble T.E., Benirschke S.K., Vedder N.B. Use of radial forearm flaps to treat complications of closed pilon fractures. J Orthop Trauma. 1992;6:358–365. - PubMed
-
- McFerran M.A., Smith S.W., Boulas H.J., Schwartz H.S. Complications encountered in the treatment of pilon fractures. J Orthop Trauma. 1992;6:195–200. - PubMed
-
- D’Alleyrand J.C., Manson T.T., Dancy L. Is time to flap coverage of open tibial fractures an independent predictor of flap-related complications. J Orthop Trauma. 2014;28:288–293. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
