

Cardiac tamponade in a patient with autoimmune polyglandular syndrome type 2
- PMID: 29062486
- PMCID: PMC5640567
- DOI: 10.1530/EDM-17-0097
Cardiac tamponade in a patient with autoimmune polyglandular syndrome type 2
Abstract
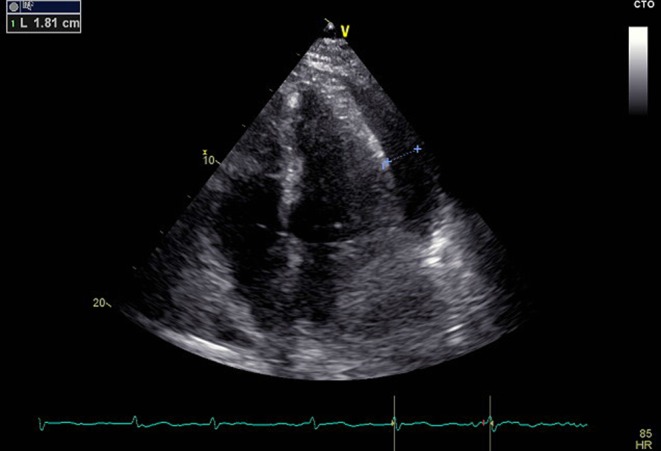
We describe a case of a 40-year-old woman who was admitted to the intensive care unit with a rapid onset of dyspnea and orthopnea. She presented progressive weakness, weight loss and secondary amenorrhea during last year, while intermittent fever was present for the last two months. Initial biochemical evaluation showed anemia, hyponatremia and increased C-reactive protein levels. Clinical and echocardiographic evaluation revealed cardiac tamponade, which was treated with pericardiocentesis. Pleural fluid samples were negative for malignancy, tuberculosis or bacterial infection. Hormonal and serologic evaluation led to the diagnosis of autoimmune polyglandular syndrome (APS) type 2 (including primary adrenal insufficiency and autoimmune thyroiditis), possibly coexisting with systemic lupus erythematosus. After symptomatic rheumatologic treatment followed by replacement therapy with hydrocortisone and fludrocortisone, the patient fully recovered. In patients with the combination of polyserositis, cardiac tamponade and persistent hyponatremia, possible coexistence of rheumatologic and autoimmune endocrine disease, mainly adrenal insufficiency, should be considered. Early diagnosis and non-invasive treatment can be life-saving.
Learning points: In patients with the combination of polyserositis, cardiac tamponade and persistent hyponatremia, possible coexistence of rheumatologic and autoimmune endocrine disease, mainly adrenal insufficiency, should be considered.Early diagnosis and non-invasive treatment can be life-saving for these patients.Primary adrenal insufficiency requires lifelong replacement therapy with oral administration of 15-25 mg hydrocortisone in split doses and 50-200 µg fludrocortisone once daily.
Keywords: 2017; ACTH; Addison's disease; Adrenal; Adrenal antibodies; Adrenal insufficiency; Adult; Amenorrhoea; Anaemia; Arthralgia; Autoimmune polyendocrine syndrome 2; Autoimmune polyglandular syndrome; C-reactive protein; Cardiac tamponade; Cardiology; Cortisol; Dyspnoea; Echocardiogram; Female; Fludrocortisone; Glucocorticoids; Greece; Hashimoto's disease; Hydrocortisone; Hyperpigmentation; Hyponatraemia; Hypotension; Levothyroxine; Methylprednisolone; Mineralocorticoids; Myasthaenia; October; Pericardial effusion; Pericardiocentesis; Pyrexia; Rash; Systemic lupus erythematosus; Tachycardia; Thyroiditis; Unique/unexpected symptoms or presentations of a disease; Weight loss; White.
Figures

References
-
- Erichsen MM, Løvas K, Skinningsrud B, Wolff AB, Undlien DE, Svartberg J, Fougner KJ, Berg TJ, Bollerslev J, Mella B, et al. 2009. Clinical, immunological, and genetic features of autoimmune primary adrenal insufficiency: observations from a Norwegian registry. Journal of Clinical Endocrinology and Metabolism 94 4882–4890. ( 10.1210/jc.2009-1368) - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
