

Evidence-based blood pressure reducing actions of electroacupuncture: mechanisms and clinical application
- PMID: 29063107
- PMCID: PMC6033058
Evidence-based blood pressure reducing actions of electroacupuncture: mechanisms and clinical application
Abstract
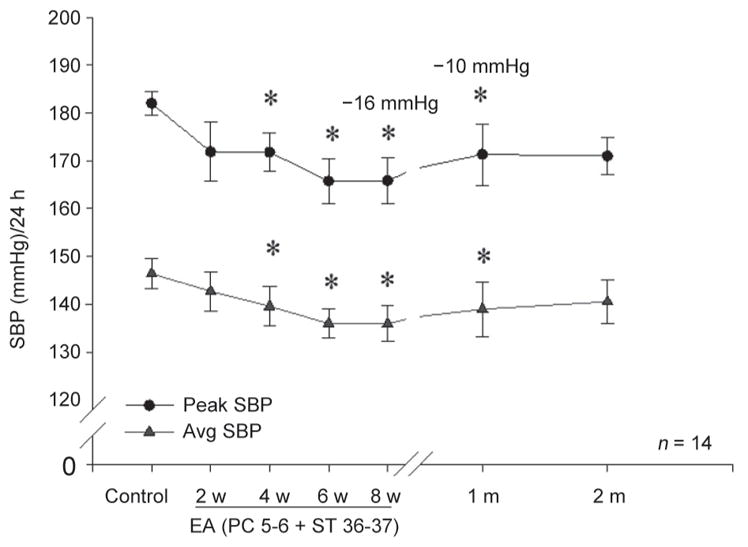
Hypertension is a serious world-wide health problem as it increases cardiovascular atherosclerotic risk, stroke and attending morbidity and mortality. Both systolic and diastolic blood pressures and particularly systolic pressure increase with aging. The downsides from pharmacological therapy have led to consideration of additional treatments, including acupuncture, which evokes endogenous neural-hormonal systems to lower blood pressure. Using basic science studies to guide clinical approaches to research, it is apparent that low frequency, low intensity electroacupuncture reduces sympathetic outflow in approximately 70% of patients with mild to moderate hypertension who are off antihypertensive drugs. Systolic and, to a lesser extent, diastolic arterial blood pressures can be lowered over two to four weeks for prolonged periods, lasting as long as one month, after cessation of an eight weeks of once weekly stimulation. Many questions about long-term therapy, treatment of resistant patients and efficacy in patients on medication remain to be studied. Current data, however, suggest that there may be a role of acupuncture in treatment of hypertension.
Figures








References
-
- Yoon SS, Carroll MD, Fryar CD. Hypertension Prevalence and Control Among Adults: United States, 2011–2014. NCHS Data Brief. 2015;(220):1–8. - PubMed
-
- Fryar CD, Chen TC, Li X. Prevalence of uncontrolled risk factors for cardiovascular disease: United States, 1999–2010. 2012;(103):1–8. - PubMed
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012;125:e2–e220. - PMC - PubMed
-
- Lewington S, Lacey B, Clarke R, Guo Y, Kong XL, Yang L, Chen Y, Bian Z, Chen J, Meng J, Xiong Y, He T, Pang Z, Zhang S, Collins R, Peto R, Li L, Chen Z. The burden of hypertension and associated risk for cardiovascular mortality in China. JAMA Intern Med. 2016;176:524–532. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
