

Assessment of immune organ dysfunction in critical illness: utility of innate immune response markers
- PMID: 29063386
- PMCID: PMC5653680
- DOI: 10.1186/s40635-017-0163-0
Assessment of immune organ dysfunction in critical illness: utility of innate immune response markers
Abstract
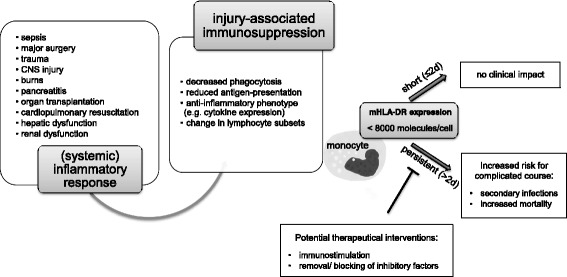
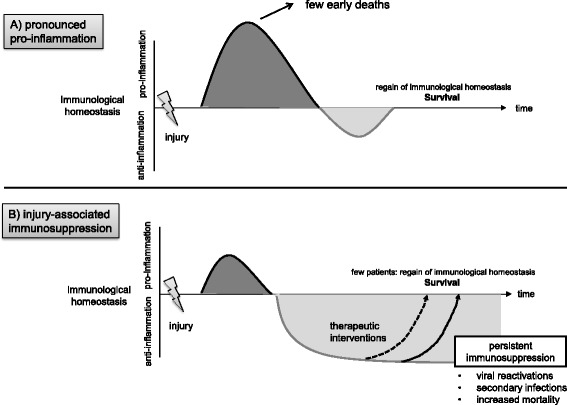
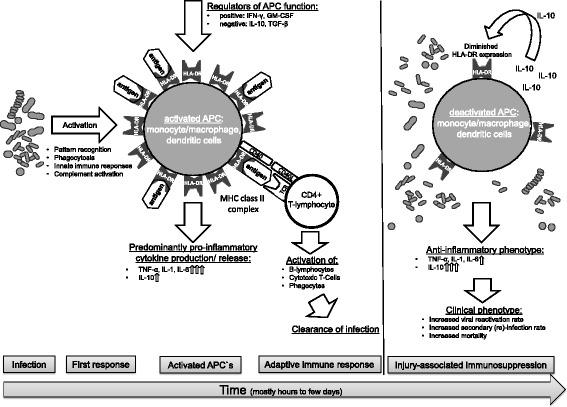
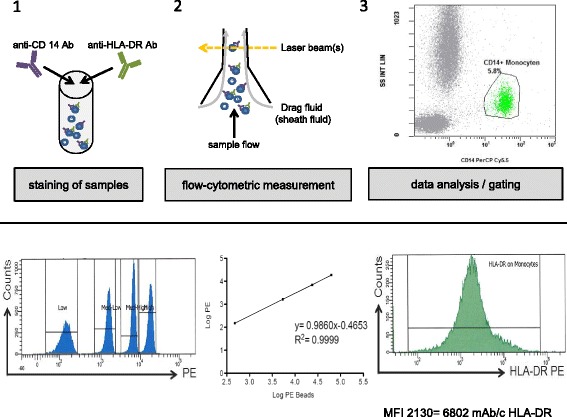
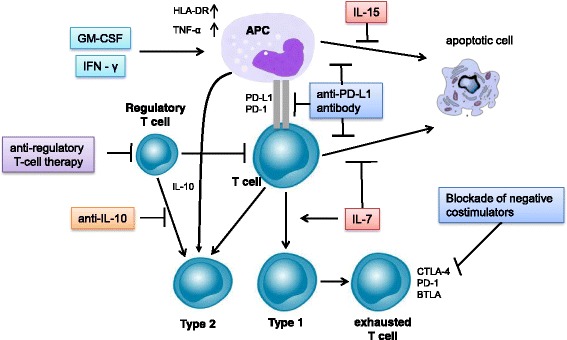
In critically ill patients, organ dysfunctions are routinely assessed, monitored, and treated. Mounting data show that substantial critical illness-induced changes in the immune system can be observed in most ICU patients and that not only "hyper-inflammation" but also persistence of an anti-inflammatory phenotype (as in sepsis-associated immunosuppression) is associated with increased morbidity and mortality. Despite common perception, changes in functional immunity cannot be adequately assessed by routine inflammatory biomarkers such as C-reactive protein, procalcitonin, or numerical analysis of leukocyte (sub)-counts. Cytokines appear also not suited due to their short half-life and pleiotropy, their unexclusive origin from immune cells, and their potential to undergo antagonization by circulating inactivating molecules. Thus, beyond leukocyte quantification and use of routine biomarkers, direct assessment of immune cell function seems required to characterize the immune systems' status. This may include determination of, e.g., ex vivo cellular cytokine release, phagocytosis activity, and/or antigen-presenting capacity. In this regard, standardized flow-cytometric assessment of the major histocompatibility-II complex human leukocyte antigen (-D related) (HLA-DR) has gained particular interest. Monocytic HLA-DR (mHLA-DR) controls the interplay between innate and adaptive immunity and may serve as a "global" biomarker of injury-associated immunosuppression, and its decreased expression is associated with adverse clinical outcomes (e.g., secondary infection risk, mortality). Importantly, recent data demonstrate that injury-associated immunosuppression can be reversed-opening up new therapeutic avenues in affected patients. Here we discuss the potential scientific and clinical value of assessment of functional immunity with a focus on monocytes/macrophages and review the current state of knowledge and potential perspectives for affected critically ill patients.
Keywords: Biomarkers; Critical illness; HLA-DR expression; Immune function; Immune modulation; Immune suppression; Immunomodulation; Sepsis; Sepsis-associated immunosuppression; mHLA-DR.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
