

Pattern Recognition of the Multiple Sclerosis Syndrome
- PMID: 29064441
- PMCID: PMC5664065
- DOI: 10.3390/brainsci7100138
Pattern Recognition of the Multiple Sclerosis Syndrome
Abstract
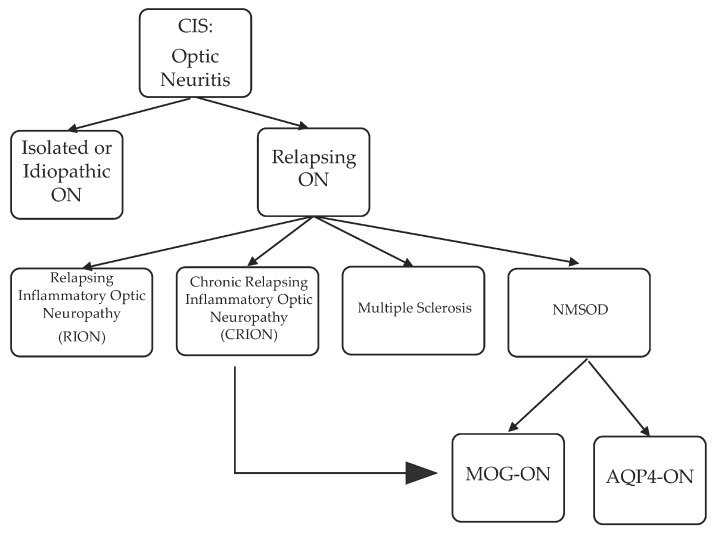
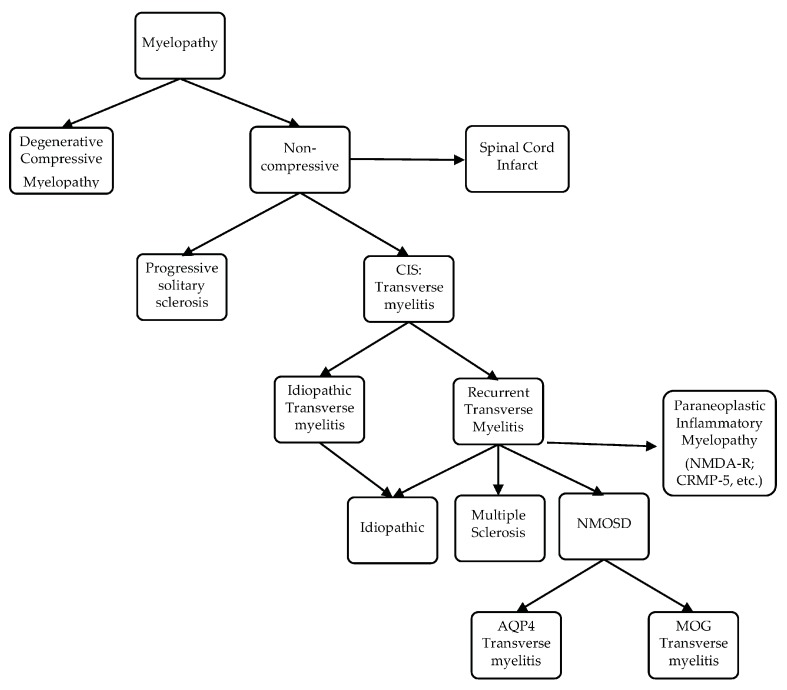
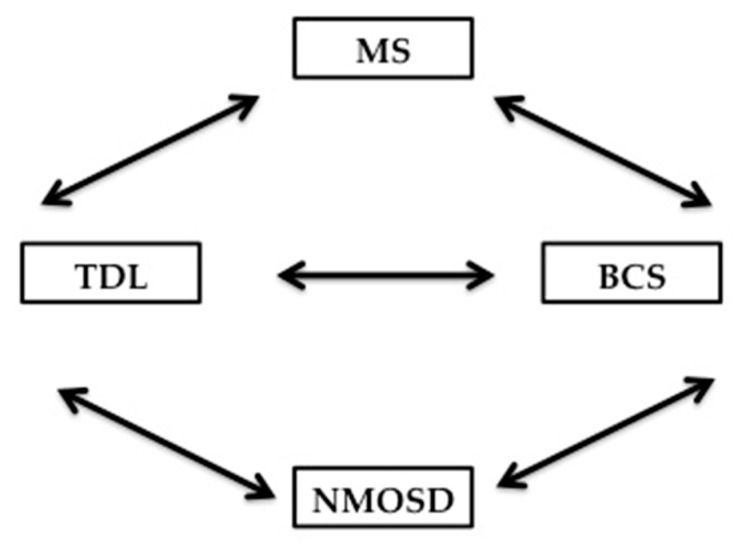
During recent decades, the autoimmune disease neuromyelitis optica spectrum disorder (NMOSD), once broadly classified under the umbrella of multiple sclerosis (MS), has been extended to include autoimmune inflammatory conditions of the central nervous system (CNS), which are now diagnosable with serum serological tests. These antibody-mediated inflammatory diseases of the CNS share a clinical presentation to MS. A number of practical learning points emerge in this review, which is geared toward the pattern recognition of optic neuritis, transverse myelitis, brainstem/cerebellar and hemispheric tumefactive demyelinating lesion (TDL)-associated MS, aquaporin-4-antibody and myelin oligodendrocyte glycoprotein (MOG)-antibody NMOSD, overlap syndrome, and some yet-to-be-defined/classified demyelinating disease, all unspecifically labeled under MSsyndrome. The goal of this review is to increase clinicians' awareness of the clinical nuances of the autoimmune conditions for MS and NMSOD, and to highlight highly suggestive patterns of clinical, paraclinical or imaging presentations in order to improve differentiation. With overlay in clinical manifestations between MS and NMOSD, magnetic resonance imaging (MRI) of the brain, orbits and spinal cord, serology, and most importantly, high index of suspicion based on pattern recognition, will help lead to the final diagnosis.
Keywords: AQP4 antibodies; MOG antibodies; MS; NMOSD; brainstem syndrome; clinically isolated syndrome (CIS); optic neuritis; transverse myelitis; tumefactive demyelinating lesions.
Conflict of interest statement
Rana K. Zabad has been a site investigator or site PI for clinical trials funded by Biogen, Genentech, Novartis, Sunpharma. In the last 2 years, she has served as a consultant for Bayer, Genzyme, TEVA Neuroscience and TG therapeutics and has given unbranded lectures sponsored by TEVA and is a member of the Adjudication Committee for a clinical trial of biotin in primary and secondary progressive multiple sclerosis sponsored by PAREXEL and medDay pharmaceutical. Renee Stewart has nothing to disclose. Kathleen Healey has received funding in the past for investigation-initiated research from the Multiple Sclerosis Foundation. In relation to this review specifically, the authors declare no conflict of interest.
Figures


References
-
- Holtje M., Mertens R., Schou M.B., Saether S.G., Kochova E., Jarius S., Pruss H., Komorowski L., Probst C., Paul F., et al. Synapsin-antibodies in psychiatric and neurological disorders: Prevalence and clinical findings. Brain Behav. Immun. 2017;66:125–134. doi: 10.1016/j.bbi.2017.07.011. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
