

JAM-A as a prognostic factor and new therapeutic target in multiple myeloma
- PMID: 29064484
- PMCID: PMC5843918
- DOI: 10.1038/leu.2017.287
JAM-A as a prognostic factor and new therapeutic target in multiple myeloma
Abstract
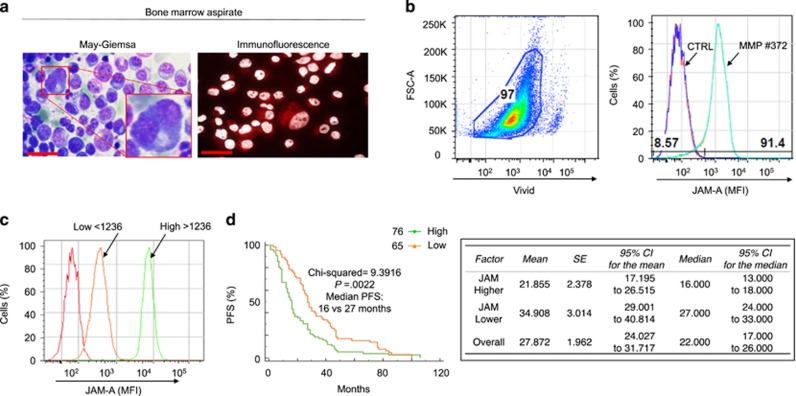
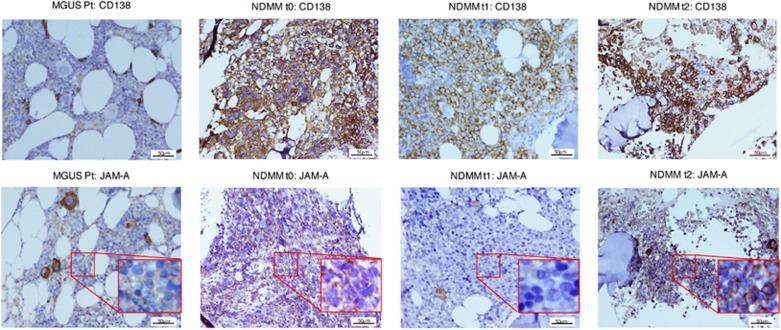
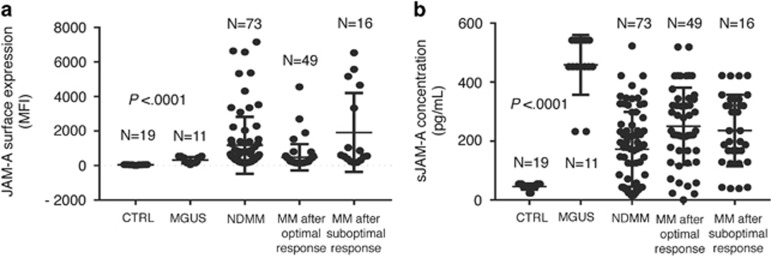
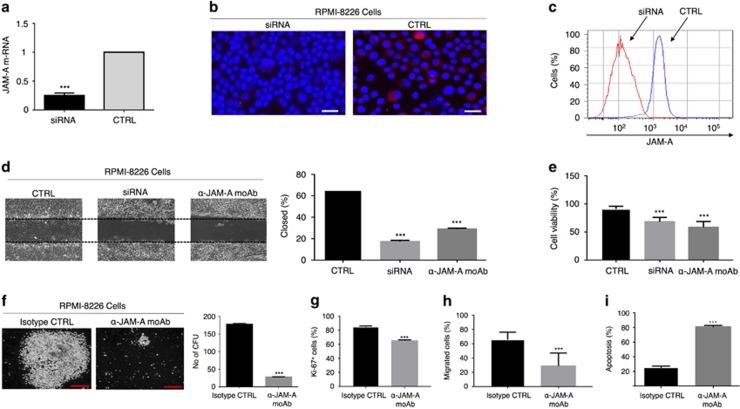
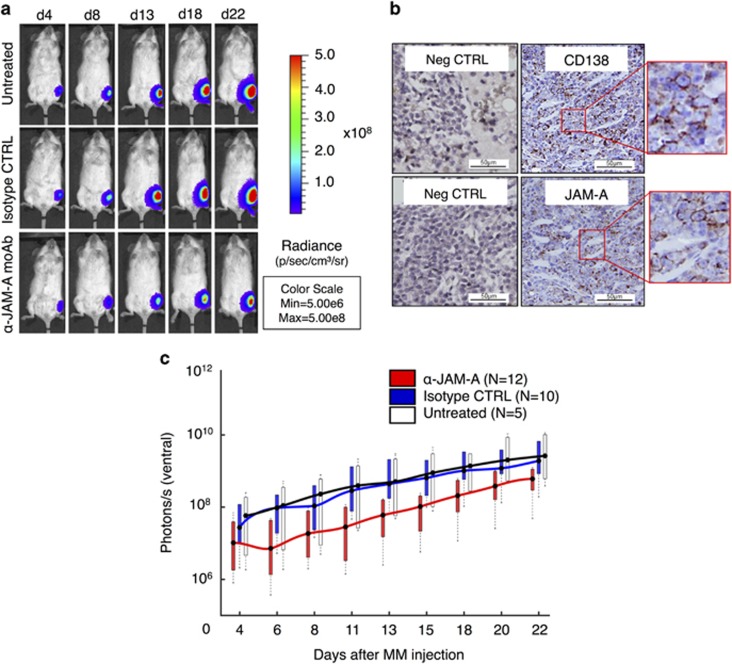
Cell adhesion in the multiple myeloma (MM) microenvironment has been recognized as a major mechanism of MM cell survival and the development of drug resistance. Here we addressed the hypothesis that the protein junctional adhesion molecule-A (JAM-A) may represent a novel target and a clinical biomarker in MM. We evaluated JAM-A expression in MM cell lines and in 147 MM patient bone marrow aspirates and biopsies at different disease stages. Elevated JAM-A levels in patient-derived plasma cells were correlated with poor prognosis. Moreover, circulating soluble JAM-A (sJAM-A) levels were significantly increased in MM patients as compared with controls. Notably, in vitro JAM-A inhibition impaired MM migration, colony formation, chemotaxis, proliferation and viability. In vivo treatment with an anti-JAM-A monoclonal antibody (αJAM-A moAb) impaired tumor progression in a murine xenograft MM model. These results demonstrate that therapeutic targeting of JAM-A has the potential to prevent MM progression, and lead us to propose JAM-A as a biomarker in MM, and sJAM-A as a serum-based marker for clinical stratification.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Mikhael JR, Dingli D, Roy V, Reeder CB, Buadi FK, Hayman SR et al. Management of newly diagnosed symptomatic multiple myeloma: updated Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) consensus guidelines 2013. Mayo Clin Proc 2013; 88: 360–376. - PubMed
-
- Mutlu P, Ural AU, Gunduz U. Differential gene expression analysis related to extracellular matrix components in drug-resistant RPMI-8226 cell line. Biomed Pharmacother Biomed Pharmacother 2012; 66: 228–231. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
